

Peritonitis - Belly on Fire
-
Inflammation of the peritoneum, the silk-like membrane lining the abdominal wall.
-
Types
- Spontaneous Bacterial Peritonitis (SBP): Infection of ascitic fluid, usually from cirrhosis. No evident source.
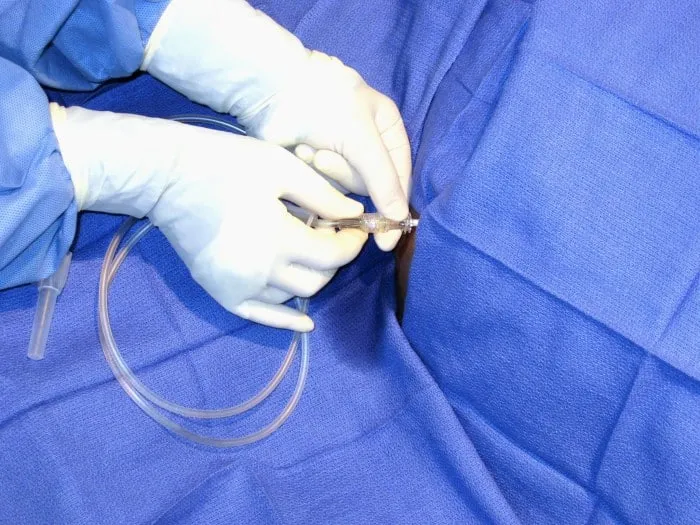
- Dx: Ascitic fluid PMN > 250 cells/mm³.
- Common bugs: E. coli, Klebsiella, Strep pneumo.
- Secondary Peritonitis: Due to perforation of a viscus (e.g., appendix, ulcer).
- Polymicrobial infection is common.
- Spontaneous Bacterial Peritonitis (SBP): Infection of ascitic fluid, usually from cirrhosis. No evident source.
-
Clinical Features
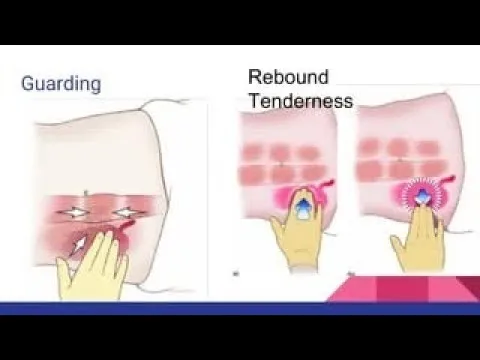
- Fever, abdominal pain, guarding, rebound tenderness.
- Classic sign: Board-like rigidity.
⭐ High-Yield: In a patient with cirrhosis, ascites, and fever, a paracentesis showing a neutrophil count (PMN) of > 250/mm³ is diagnostic for SBP.
SBP - Cirrhosis's Sneaky Friend
- Definition: Bacterial infection of ascitic fluid without an evident intra-abdominal source, common in advanced cirrhosis.
- Etiology: Primarily monomicrobial. Gram-negative bacilli are most frequent, especially E. coli (~70%), Klebsiella, and Streptococcus species.
- Clinical: Can be subtle. Look for fever, abdominal pain, and altered mental status (worsening hepatic encephalopathy).
- Diagnosis: Requires paracentesis. Key finding is an ascitic fluid absolute neutrophil count (PMN) $≥ \textbf{250}/mm^3$.
- Management:
- Empiric antibiotics (e.g., 3rd-gen cephalosporin like cefotaxime).
- IV albumin infusion.
⭐ High-Yield: Initiate treatment based on a PMN count $≥ \textbf{250}/mm^3$ alone. Do not wait for culture results, as they have low sensitivity and delay can be fatal.
Secondary Peritonitis - The Great Escape
- Pathophysiology: Breach of GI/GU tract integrity → spillage of polymicrobial gut flora into the normally sterile peritoneal cavity.
- Common Causes: Perforated peptic ulcer, acute appendicitis, diverticulitis, trauma, or iatrogenic injury.
- Microbiology: Mixed aerobes (E. coli, Klebsiella) and anaerobes (Bacteroides fragilis).
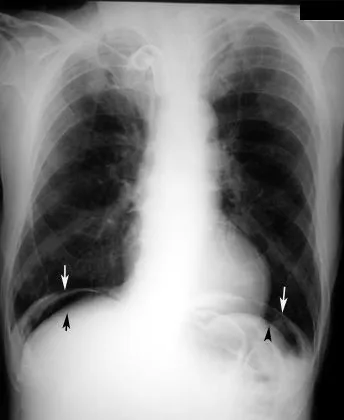
- Diagnosis: Clinical signs of an acute abdomen (rebound tenderness, guarding). Upright CXR or CT scan confirms pneumoperitoneum (free air).
⭐ Bacteroides fragilis is the most common anaerobe isolated, mandating antibiotic coverage for anaerobes.
Dx & Tx - Find It, Fix It
-
Find It (Diagnosis):
- Labs: CBC (↑ WBC), blood cultures.
- Paracentesis (if ascites): Ascitic fluid PMN count > 250 cells/mm³ is diagnostic for SBP.
- Imaging: Upright X-ray (free air) or CT scan (abscess, definitive source).
-
Fix It (Treatment Algorithm):
⭐ For Spontaneous Bacterial Peritonitis (SBP), treatment is empiric antibiotics (e.g., 3rd-gen cephalosporin). Surgical intervention is typically NOT indicated, unlike secondary peritonitis.
High‑Yield Points - ⚡ Biggest Takeaways
- Spontaneous Bacterial Peritonitis (SBP) is a key complication of cirrhosis and ascites, most commonly caused by E. coli. Diagnosis requires >250 neutrophils/mm³ in ascitic fluid.
- Secondary peritonitis results from bowel perforation (e.g., appendicitis, diverticulitis) and is typically polymicrobial.
- Peritoneal dialysis (PD)-associated peritonitis is often caused by skin flora like Staph aureus.
- Classic signs include diffuse abdominal pain, rebound tenderness, and guarding.
- Tuberculous peritonitis can present insidiously with a "doughy" abdomen and high ascitic fluid ADA.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more