

Conduction System - The Heart's Electrical Grid
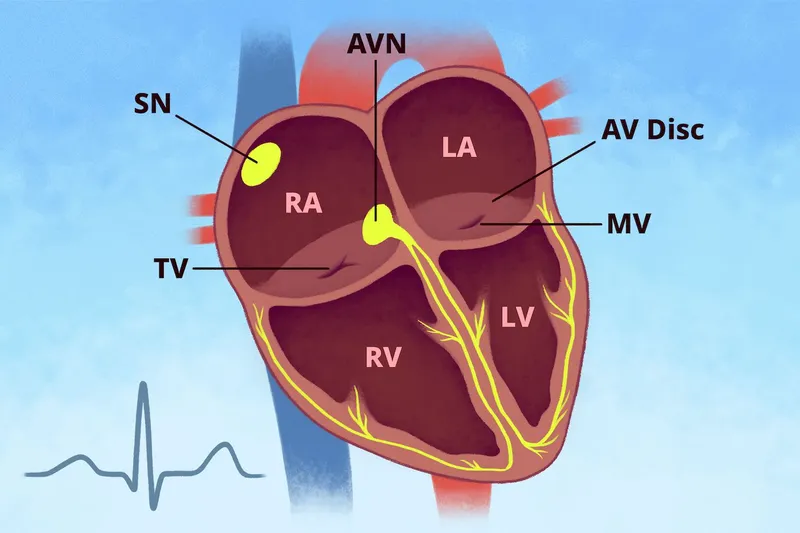
- Pacemaker Hierarchy: The heart's electrical signal originates and travels through specialized tissue.
- Sinoatrial (SA) node: Primary pacemaker (60-100 bpm).
- Atrioventricular (AV) node: Gatekeeper to ventricles (40-60 bpm).
- His-Purkinje system: Final pathway (20-40 bpm).
⭐ The AV node physiologically delays the impulse (~0.12s), allowing ventricles to fill completely before contraction. This delay creates the PR interval on an ECG.
AV Blocks - Communication Breakdown
- Pathophysiology: Delay or interruption of the electrical signal from the atria to the ventricles at the AV node or His-Purkinje system.
| Type | ECG Findings | Clinical Significance |
|---|---|---|
| 1st Degree | Fixed, prolonged PR interval (>0.20s). Every P wave is followed by a QRS. | Usually benign and asymptomatic. |
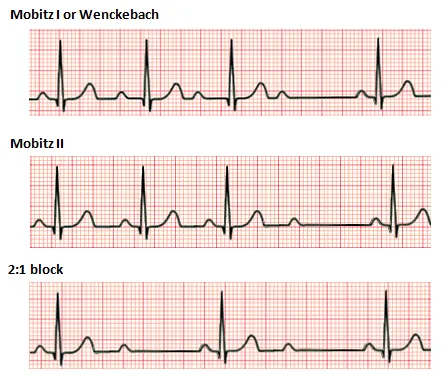
| 2nd Degree (Mobitz I) | Progressive PR lengthening until a QRS complex is dropped. | 📌 "Longer, longer, drop, then you have a Wenckebach." Low risk. |
| 2nd Degree (Mobitz II) | Constant PR interval with intermittent, unexpected dropped QRS complexes. | High risk of progression to 3rd-degree block. Pacemaker indicated. |
| 3rd Degree (Complete) | Complete AV dissociation; P waves and QRS complexes act independently. | Medical emergency. Requires immediate pacing due to risk of asystole. |
Bundle Branch Blocks - Signal Detours
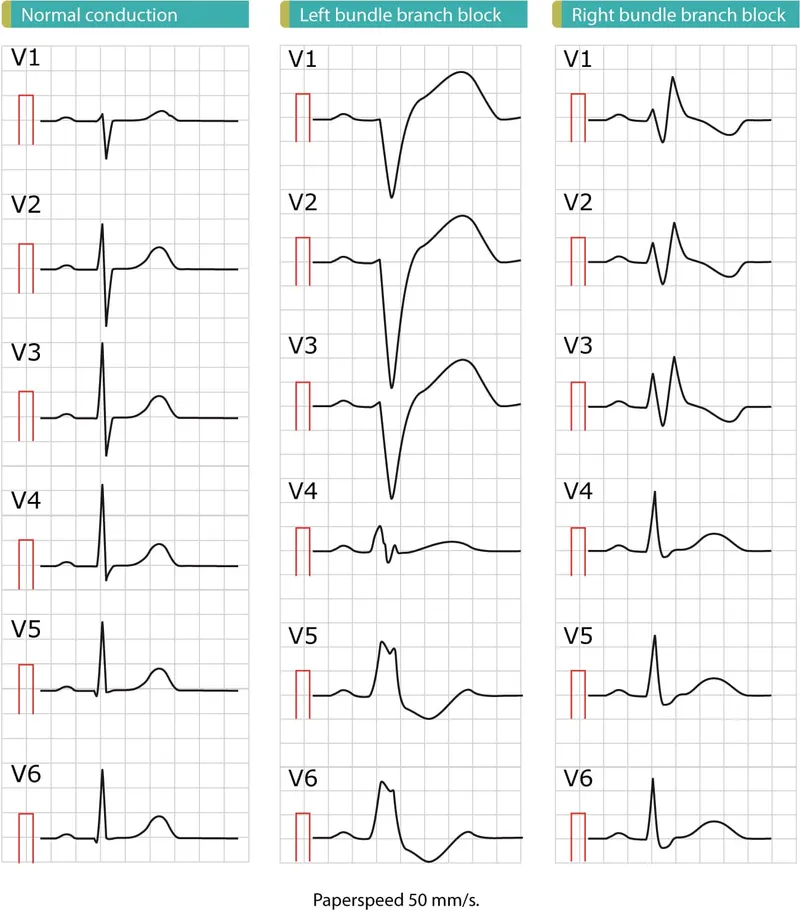
- Pathophysiology: Conduction delay or block in the right or left bundle branch, widening the QRS complex to > 0.12s.
- Right Bundle Branch Block (RBBB):
- ECG: RSR' pattern ("rabbit ears") in leads V1-V2; wide, slurred S wave in leads I, aVL, V5-V6.
- Often benign in asymptomatic individuals.
- Left Bundle Branch Block (LBBB):
- ECG: Broad, notched, or slurred R wave in I, aVL, V5-V6; deep S wave in V1-V3.
- Often indicates underlying cardiac disease.
⭐ A new LBBB in the context of chest pain should be treated as a STEMI equivalent.
📌 Mnemonic (WiLLiaM MaRRoW):
- In LBBB, see W-shape in V1 & M-shape in V6.
- In RBBB, see M-shape in V1 & W-shape in V6.
Management - When to Shock or Pace
- Assess Stability: First, determine if bradycardia is causing hemodynamic instability (hypotension, altered mental status, shock, chest pain, acute heart failure).
⭐ For high-degree AV blocks (Mobitz II, Third-Degree), transcutaneous pacing should be immediately prepared and is preferred over atropine, which may be ineffective or even paradoxical.
High‑Yield Points - ⚡ Biggest Takeaways
- Sick Sinus Syndrome often presents as tachy-brady syndrome, causing syncope or dizziness in the elderly.
- Mobitz II and Third-Degree (Complete) AV Block are high-risk for asystole and require a permanent pacemaker.
- Mobitz I (Wenckebach) shows progressive PR prolongation before a dropped QRS; it is typically benign.
- Third-Degree Block is defined by complete AV dissociation (P waves and QRS complexes are independent).
- Atropine is first-line for symptomatic bradycardia; use transcutaneous pacing if unresponsive or for high-degree blocks.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more