

NF-κB Overview - The Cell's First Responder
- A rapid-acting transcription factor central to immunity, inflammation, and cell survival.
- Normally sequestered in the cytoplasm in an inactive state, bound to its inhibitor, IκB.
- Activated by a vast range of stimuli, including:
- PAMPs: LPS (via TLRs)
- Pro-inflammatory cytokines: TNF-α, IL-1
⭐ High-Yield: Overactivation of NF-κB is a key factor in the pathogenesis of septic shock (due to massive cytokine release) and contributes to many chronic inflammatory diseases like rheumatoid arthritis and inflammatory bowel disease.
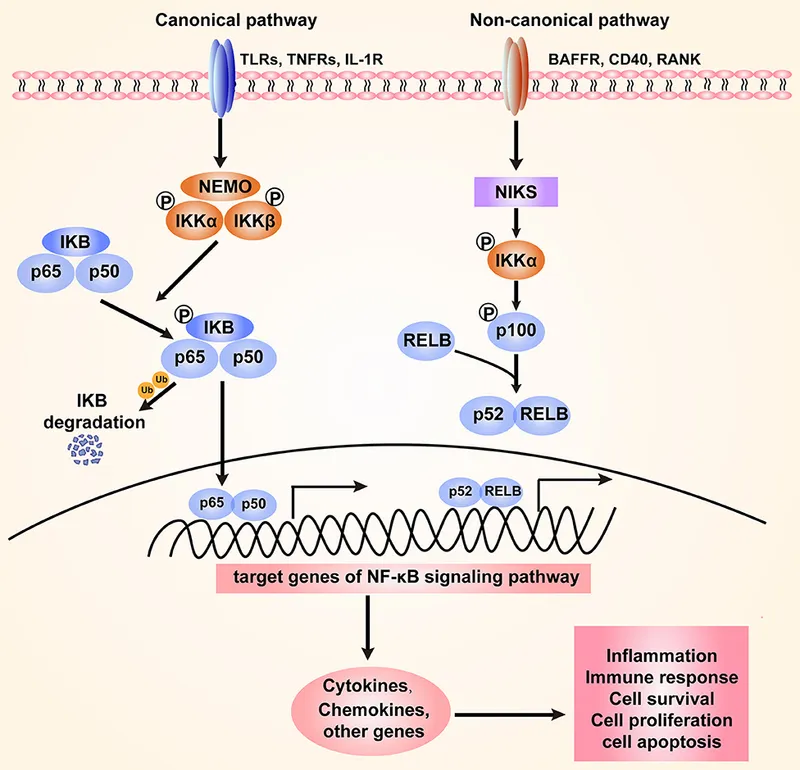
Canonical Pathway - The Main Activation Route
- Trigger: Pro-inflammatory cytokines (e.g., TNF-α, IL-1), antigens, or Pathogen-Associated Molecular Patterns (PAMPs).
- Resting State: NF-κB (typically p65/p50 heterodimer) is sequestered in the cytoplasm, bound to its inhibitor, IκBα.
- Activation Cascade:
- Signal binding activates the IκB Kinase (IKK) complex.
- IKK phosphorylates IκBα, marking it for ubiquitination and proteasomal degradation.
- 📌 In Kase of Krisis, Inκrease Burning (IKK phosphorylates IκB).
- Freed NF-κB translocates to the nucleus, binding to κB sites on DNA to initiate gene transcription.
⭐ The pro-inflammatory cytokines TNF-α and IL-1 are potent activators of the canonical NF-κB pathway, a central mechanism in acute inflammation and sepsis.
Clinical Relevance - Disease & Drug Targets
-
Overactive NF-κB is a key driver in many human diseases due to its pro-inflammatory and pro-survival signaling.
- Chronic Inflammatory Disorders: Implicated in Rheumatoid Arthritis, Inflammatory Bowel Disease (IBD), and psoriasis.
- Cancer: Contributes to oncogenesis by promoting cell proliferation, angiogenesis, and metastasis while inhibiting apoptosis.
-
Pharmacological Inhibitors as Drug Targets:
| Drug Class | Mechanism on NF-κB Pathway | Clinical Example |
|---|---|---|
| Glucocorticoids | Upregulate the gene for IκBα, enhancing its inhibitory effect. | Prednisone |
| Proteasome Inhibitors | Block IκBα degradation, preventing NF-κB nuclear translocation. | Bortezomib |
| NSAIDs (High-Dose) | Aspirin can inhibit IκK activity, reducing phosphorylation of IκBα. | Aspirin |
High‑Yield Points - ⚡ Biggest Takeaways
- NF-κB is a master transcription factor for the inflammatory response.
- In its inactive state, it is sequestered in the cytoplasm by its inhibitor, IκB.
- Activation by signals like TNF-α or IL-1 leads to phosphorylation of IκB by the IKK complex.
- Phosphorylated IκB is targeted for ubiquitination and proteasomal degradation.
- This releases NF-κB, allowing it to translocate to the nucleus and activate gene transcription.
- Aberrant NF-κB signaling is a hallmark of many chronic inflammatory diseases and cancers.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more