

Skull & C-Spine Landmarks - Head Turner Views
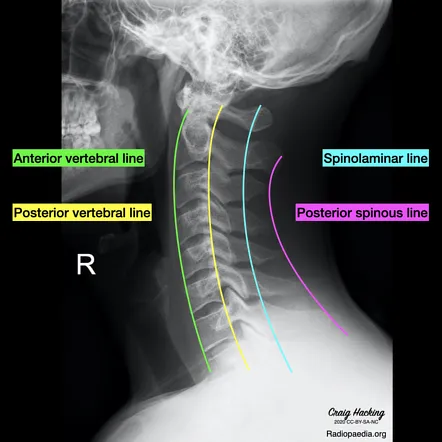
- Lateral View: Key for assessing alignment and soft tissues. Check for three smooth, parallel curves:
- Anterior vertebral line
- Posterior vertebral line
- Spinolaminar line
- Odontoid (Open-Mouth) View: Visualizes C1-C2 articulation.
- Lateral masses of C1 must align with the superior articular facets of C2.
- Swimmer's View: Used when the C7-T1 junction is not visible on the lateral view.
⭐ The normal atlantodental interval (ADI) is <3 mm in adults and <5 mm in children. An increased distance suggests transverse ligament rupture, often seen in trauma or rheumatoid arthritis.
Thorax & Spine Landmarks - Rib-Tickling Reads
- Sternal Angle (of Louis): Palpable ridge on the sternum. Key landmark for the 2nd rib.
- Carina: Bifurcation of the trachea, typically at the T4-T5 vertebral level.
- Aortic Knob/Arch: Prominent shadow on chest X-ray, arching over the left pulmonary artery, also at T4 level.
- Diaphragmatic Openings:
- 📌 Mnemonic "I Ate Ten Eggs At Twelve" (IVC at T8, Esophagus at T10, Aorta at T12).
- Costophrenic Angles: Sharp, acute angles where diaphragm meets ribs on a PA chest X-ray. Blunting suggests effusion.
⭐ The Sternal Angle of Louis is a crucial clinical landmark. It corresponds to the level of the T4/T5 intervertebral disc, the bifurcation of the trachea (carina), and the beginning/end of the aortic arch.
Pelvis & Hip Landmarks - Hip, Hip, Hooray!
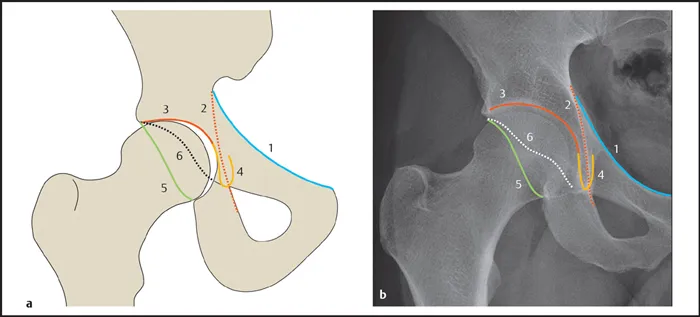
- Key Lines for Hip Assessment (AP View):
- Hilgenreiner's Line: Horizontal line through bilateral triradiate cartilages.
- Perkin's Line: Vertical line perpendicular to Hilgenreiner's at the lateral acetabular margin.
- Shenton's Line: A continuous, smooth arc from the medial femoral neck to the inferior pubic ramus.
- Klein's Line: Drawn along the superior border of the femoral neck; femoral head should intersect it. Crucial for SCFE diagnosis.
- Key Angles:
- Acetabular Angle: Formed by Hilgenreiner's line and acetabular roof. Normal: <30° at birth.
⭐ A disrupted Shenton's line is a key indicator of a femoral neck fracture or developmental dysplasia of the hip (DDH).
Extremity Landmarks - Joint Venture Views
- Shoulder (AP/Axillary/Y-view): Check glenohumeral alignment.
- Elbow (AP/Lateral): Anterior humeral & radiocapitellar lines. Posterior fat pad sign indicates occult fracture.
- Wrist (AP/Lateral/Scaphoid): Look for scapholunate dissociation; gap >3 mm is abnormal.
- Hip (AP/Frog-leg): Trace Shenton's line for femoral neck fracture.
- Ankle (AP/Lateral/Mortise): Mortise view is critical for assessing joint space integrity.
⭐ Posterior Shoulder Dislocation: Often missed on AP view; humeral head appears symmetric ("lightbulb sign"). Axillary view is crucial for diagnosis.
High-Yield Points - ⚡ Biggest Takeaways
- C1 (Atlas) is distinguished by its lack of a vertebral body and spinous process.
- The dens (odontoid process) is the key identifier for the C2 vertebra (Axis).
- Vertebra prominens (C7) provides a critical palpable landmark with its long spinous process.
- The scaphoid, located in the anatomic snuffbox, is the most commonly fractured carpal bone.
- Sella turcica is a depression in the sphenoid bone that houses the pituitary gland.
- The carina marks the tracheal bifurcation, typically found at the T4-T5 vertebral level.
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more