
Hand Surgery

On this page
🏗️ Hand Surgery: The Precision Engineering Marvel
The hand contains more than a quarter of your body's bones orchestrated through an intricate network of tendons, nerves, and vessels-making it both a biomechanical marvel and a diagnostic challenge. You'll master the systematic approach surgeons use to evaluate hand injuries and conditions, learning to recognize injury patterns, build differential diagnoses, and select evidence-based treatments. This lesson transforms complex anatomy into actionable clinical frameworks, equipping you with the pattern recognition and decision algorithms that separate competent evaluation from expert care.

The hand represents the pinnacle of evolutionary engineering, where millimeter-precise anatomical relationships determine the difference between normal function and devastating disability. Understanding hand surgery requires mastering this complex three-dimensional architecture where tendon excursions of 5-7cm translate into 90-degree joint motion, and where nerve territories overlap by 2-3mm creating critical zones for surgical decision-making.
📌 Remember: SOME LOVERS TRY POSITIONS THAT THEY CAN'T HANDLE - Scaphoid, Lunate, Triquetrum, Pisiform, Trapezium, Trapezoid, Capitate, Hamate (proximal to distal, radial to ulnar carpal arrangement)
Hand surgery encompasses the management of trauma affecting 15% of emergency presentations, congenital anomalies occurring in 1:2,500 births, and degenerative conditions affecting 25% of adults over 50. The specialty demands understanding of microsurgical techniques with vessel anastomosis success rates of 95%, nerve repair protocols achieving meaningful recovery in 70-80% of cases, and tendon reconstruction restoring 80-90% of normal strength.
| Structure | Quantity | Clinical Significance | Repair Timeline | Success Rate |
|---|---|---|---|---|
| Bones | 27 | Fracture healing 6-12 weeks | Non-union risk 5-10% | Union rate 90-95% |
| Joints | 29 | ROM loss 10-20% post-injury | Stiffness prevention critical | Functional recovery 80% |
| Tendons | 34 muscles | Zone II repairs most challenging | Healing 6-8 weeks | Good results 75-85% |
| Nerves | 3 major | Regeneration 1mm/day | Recovery 6-18 months | Useful function 70% |
| Vessels | 2 arterial arches | Collateral circulation critical | Immediate patency required | Patency rate 95% |
⭐ Clinical Pearl: Allen's test demonstrates ulnar artery dominance in 80% of hands - critical for radial artery harvest procedures where completion time >7 seconds indicates inadequate ulnar circulation
- Skeletal Framework Architecture
- Proximal row: Scaphoid, lunate, triquetrum, pisiform
- Scaphoid fractures: 10% of all fractures, non-union risk 15%
- Lunate dislocations: Mayfield classification stages I-IV
- Distal row: Trapezium, trapezoid, capitate, hamate
- Hamate hook fractures: Athletes 60%, non-union common
- Capitate: Central keystone, AVN risk with fracture
- Metacarpals: 5 bones with unique biomechanics
- Boxer's fracture: 5th metacarpal neck, angulation <40 degrees acceptable
- Bennett fracture: 1st metacarpal base, requires ORIF
- Proximal row: Scaphoid, lunate, triquetrum, pisiform
💡 Master This: Zone II flexor tendon injuries ("no man's land") have historically poor outcomes due to tendon sheath constraints and adhesion formation - modern two-strand repair techniques with early mobilization protocols achieve good-excellent results in 75-85% of cases
The tendon system operates through precise excursion ratios where FDP tendons travel 7cm to achieve full finger flexion, while FDS tendons contribute 5cm excursion for PIP joint motion. Understanding these biomechanical relationships guides surgical repair techniques and rehabilitation protocols essential for optimal functional outcomes.
Connect these foundational anatomical principles through biomechanical analysis to understand how structural relationships determine surgical approaches and functional restoration strategies.
🏗️ Hand Surgery: The Precision Engineering Marvel


⚙️ Biomechanical Powerhouse: The Hand's Motion Engine
The hand's kinetic chain functions through intricate muscle balance where intrinsic muscles provide precision control while extrinsic muscles generate power grip forces up to 400N. Flexor digitorum profundus produces individual finger flexion with force generation of 80-120N per digit, while flexor digitorum superficialis contributes PIP joint flexion with independent finger control in 85% of individuals.
📌 Remember: FDS INDEPENDENCE TEST - Middle finger most independent (95%), Ring finger least independent (25%), Index and little finger intermediate (60-70%)
Loading diagram…
Grip patterns demonstrate sophisticated neural control where power grip engages all digits with thumb opposition generating combined forces of 300-500N, while precision pinch utilizes thumb-index coordination producing forces of 50-80N with positional accuracy of 1-2mm. These biomechanical patterns require intact sensory feedback from mechanoreceptors providing position sense and force modulation.
| Grip Type | Force Generated | Muscles Involved | Clinical Testing | Pathology Impact |
|---|---|---|---|---|
| Power Grip | 300-500N | All flexors + thumb | Dynamometer testing | Median nerve: 50% loss |
| Precision Pinch | 50-80N | FPL, FDP index, thenar | Pinch meter | Ulnar nerve: 60% loss |
| Lateral Pinch | 80-120N | FPL, adductor pollicis | Key pinch test | Combined: 80% loss |
| Tip Pinch | 40-60N | FPL, FDP, lumbricals | O-ring test | Intrinsic loss: 40% loss |
| Cylindrical Grip | 200-300N | All flexors | Grip span test | Flexor loss: 90% loss |
⭐ Clinical Pearl: Pulley reconstruction using palmaris longus grafts achieves 90% strength restoration when A2 and A4 pulleys are reconstructed, but isolated A2 reconstruction provides only 60% mechanical efficiency
- Intrinsic-Extrinsic Balance Mechanisms
- Intrinsic muscles: Precision control and MCP flexion
- Lumbricals: MCP flexion + IP extension, force 15-20N each
- Interossei: Finger abduction/adduction, force 25-35N each
- Extrinsic flexors: Power generation and grip strength
- FDP: DIP flexion, excursion 7cm, force 80-120N per digit
- FDS: PIP flexion, excursion 5cm, force 60-90N per digit
- Extrinsic extensors: Finger extension and wrist stabilization
- EDC: MCP extension, force 40-60N per digit
- EPL/EPB: Thumb extension, critical for pinch stability
- Intrinsic muscles: Precision control and MCP flexion
💡 Master This: Intrinsic muscle paralysis creates claw deformity with MCP hyperextension and IP flexion because extrinsic extensors cannot extend IP joints without intrinsic muscle balance - tendon transfers restore function in 80-85% of cases
Sensory integration provides critical feedback for motor control where two-point discrimination of 2-5mm in fingertips enables fine manipulation. Median nerve supplies precision grip sensation while ulnar nerve provides power grip feedback - combined sensory loss reduces hand function by 70-80%.
Understanding these biomechanical principles through clinical correlation patterns reveals how injury mechanisms disrupt functional relationships and guides surgical reconstruction strategies.
⚙️ Biomechanical Powerhouse: The Hand's Motion Engine

🎯 Pattern Recognition Mastery: Clinical Decision Framework
Injury pattern recognition follows predictable anatomical relationships where high-energy trauma creates multiple structure involvement in 70% of cases, while low-energy injuries typically affect single structures in 80% of presentations. Glass lacerations cause clean tendon divisions with repair success rates of 85-90%, while crush injuries create zone of injury extending 2-3cm beyond visible damage with complication rates of 30-40%.
📌 Remember: GLASS CUTS CLEAN, CRUSH KILLS CELLS - Glass lacerations: sharp division, minimal tissue damage, excellent repair potential; Crush injuries: extensive tissue damage, compromised vascularity, high complication rates
Systematic examination protocols identify injury patterns through sequential assessment where inspection reveals obvious deformity in 60% of fractures, palpation localizes tenderness to specific structures, and functional testing demonstrates deficit patterns characteristic of anatomical damage. Missed injuries occur in 15-20% of complex trauma when systematic protocols are not followed.
- Trauma Pattern Recognition Framework
- High-energy mechanisms: Motor vehicle accidents, industrial injuries
- Multiple structure involvement: Bone + tendon + nerve in 70%
- Compartment syndrome risk: Pressure >30mmHg requires fasciotomy
- Amputation consideration: MESS score >7 predicts poor salvage
- Low-energy mechanisms: Lacerations, simple falls
- Single structure injury: Isolated tendon or nerve in 80%
- Primary repair feasible: Success rates 85-95%
- Early mobilization possible: Rehabilitation starts 3-5 days
- Penetrating injuries: Glass, knife wounds
- Zone of injury assessment: Damage extends 1-2cm beyond visible wound
- Neurovascular evaluation: Allen's test, two-point discrimination
- Tendon testing: Individual muscle function assessment
- High-energy mechanisms: Motor vehicle accidents, industrial injuries
Loading diagram…
| Clinical Sign | Structure Involved | Sensitivity | Specificity | Management Priority |
|---|---|---|---|---|
| Tenodesis Loss | Flexor tendons | 95% | 90% | Immediate repair |
| Boutonniere Deformity | Central slip | 85% | 95% | Splinting vs surgery |
| Mallet Finger | Terminal extensor | 100% | 100% | Conservative first |
| Thenar Atrophy | Median nerve | 80% | 95% | Urgent exploration |
| Claw Deformity | Ulnar nerve | 90% | 85% | Tendon transfers |
⭐ Clinical Pearl: Scaphoid fractures show initial X-ray sensitivity of only 70% - clinical suspicion with anatomical snuffbox tenderness requires immobilization and repeat imaging at 10-14 days or immediate MRI for definitive diagnosis
Functional deficit patterns predict surgical outcomes where complete tendon divisions achieve good-excellent results in 80-85% with primary repair, partial tendon injuries may progress to rupture in 30% of cases without surgical intervention, and nerve injuries require immediate exploration when two-point discrimination exceeds 15mm in critical sensory areas.
💡 Master This: Zone II flexor tendon injuries require immediate recognition because delayed repair beyond 7-10 days reduces success rates from 85% to 60% due to tendon retraction and sheath scarring - early mobilization protocols starting day 3-5 prevent adhesion formation
Understanding these recognition patterns through systematic differential analysis enables rapid triage decisions and optimal treatment sequencing for complex hand injuries.
🎯 Pattern Recognition Mastery: Clinical Decision Framework


🔬 Systematic Analysis: Differential Diagnosis Architecture
Differential diagnosis frameworks systematically distinguish similar presentations through quantitative discriminators where infection presents with WBC >12,000 and ESR >50mm/hr in 80% of cases, inflammatory arthritis shows morning stiffness >60 minutes with symmetric joint involvement, and mechanical problems demonstrate consistent ROM limitations without systemic symptoms.
📌 Remember: SITE HELPS DIAGNOSE - Swelling pattern, Inflammatory markers, Temperature changes, Erythema distribution - History timeline, End-feel quality, Location specificity, Pain characteristics, Symmetry assessment
Tendon injury differentiation requires precise functional testing where FDP testing isolates DIP flexion with PIP joint held extended, FDS testing blocks adjacent fingers to eliminate FDP contribution, and extensor testing evaluates individual tendon function through specific finger positioning. Partial tendon injuries maintain weak function in 60% of cases but progress to complete rupture in 30% without surgical intervention.
| Condition | Pain Pattern | ROM Limitation | Inflammatory Markers | Imaging Findings | Treatment Response |
|---|---|---|---|---|---|
| Infection | Throbbing, severe | Painful restriction | WBC >12K, ESR >50 | Fluid collections | Antibiotics 48-72hrs |
| Arthritis | Morning stiffness | Symmetric loss | RF+, CRP elevated | Joint space narrowing | DMARDs weeks-months |
| Tendon Adhesions | Mechanical pain | Passive > active | Normal markers | Tendon thickening | Therapy 6-12 weeks |
| Joint Contracture | End-range pain | Passive = active | Normal markers | Capsular thickening | Surgery if >6 months |
| Nerve Compression | Numbness/tingling | Normal ROM | Normal markers | Nerve swelling | Splinting 6-12 weeks |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | |||||
| flowchart TD |
Start["✋ Hand Stiffness
• Chief complaint• Hand evaluation"]
TimeCol["📋 Duration?
• Acute vs Chronic• Timeline check"]
Inflam["⚠️ Inflammation?
• Redness/Swelling• Local heat signs"]
Passive["📋 Passive ROM?
• Range of motion• Joint movement"]
InfArth["🩺 Infection/Arthritis
• Septic joint?• Inflam. arthritis"]
TrauOver["🩺 Trauma/Overuse
• Injury history• Repetitive strain"]
JointCon["🩺 Joint Contracture
• Capsule stiffness• Fixed deformity"]
TenAdh["🩺 Tendon Adhesion
• Gliding issue• Scarring nodes"]
LabCult["🔬 Labs + Culture
• CBC and ESR/CRP• Synovial fluid"]
ImgFunc["🔬 Imaging/Testing
• X-ray or Ultrasound• Functional exam"]
SurgRel["💊 Surgical Release
• Capsulotomy• Joint procedure"]
Tenolysis["💊 Tenolysis Plan
• Tendon release• Post-op therapy"]
Start --> TimeCol TimeCol -->|< 6 weeks| Inflam TimeCol -->|> 6 months| Passive
Inflam -->|Yes| InfArth Inflam -->|No| TrauOver
Passive -->|Limited| JointCon Passive -->|Normal| TenAdh
InfArth --> LabCult TrauOver --> ImgFunc JointCon --> SurgRel TenAdh --> Tenolysis
style Start fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style TimeCol fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style Inflam fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style Passive fill:#FEF8EC, stroke:#FBECCA, stroke-width:1.5px, rx:12, ry:12, color:#854D0E style InfArth fill:#FDF4F3, stroke:#FCE6E4, stroke-width:1.5px, rx:12, ry:12, color:#B91C1C style TrauOver fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style JointCon fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style TenAdh fill:#F7F5FD, stroke:#F0EDFA, stroke-width:1.5px, rx:12, ry:12, color:#6B21A8 style LabCult fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C style ImgFunc fill:#FFF7ED, stroke:#FFEED5, stroke-width:1.5px, rx:12, ry:12, color:#C2410C style SurgRel fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534 style Tenolysis fill:#F1FCF5, stroke:#BEF4D8, stroke-width:1.5px, rx:12, ry:12, color:#166534
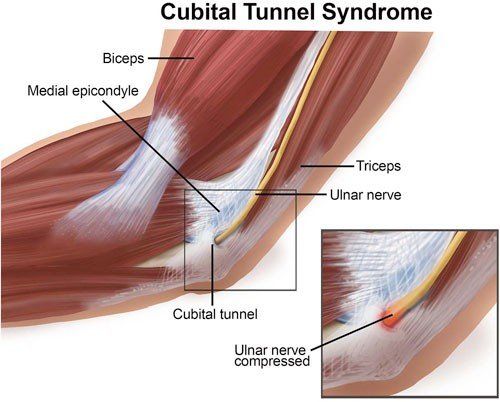
**Nerve compression syndromes** demonstrate **characteristic patterns** where **carpal tunnel syndrome** causes **median nerve symptoms** with **nocturnal pain** in **80% of cases**, **cubital tunnel syndrome** affects **ulnar nerve** with **elbow flexion aggravation**, and **radial tunnel syndrome** creates **posterior interosseous nerve** symptoms without **sensory loss**. **Electrodiagnostic studies** confirm **diagnosis** with **sensitivity 85-95%** when **clinical suspicion** is **moderate to high**.
* **Systematic Discrimination Criteria**
- **Infectious vs Inflammatory Arthritis**
+ **Infection**: **Unilateral**, **acute onset**, **fever 60%**, **WBC >15K**
+ **Arthritis**: **Bilateral**, **gradual onset**, **morning stiffness**, **RF+ 70%**
- **Tendon Adhesions vs Joint Contracture**
+ **Adhesions**: **Passive ROM > active ROM**, **tendon gliding loss**
+ **Contracture**: **Passive ROM = active ROM**, **capsular end-feel**
- **Acute vs Chronic Nerve Compression**
+ **Acute**: **Sudden onset**, **severe symptoms**, **surgical urgency**
+ **Chronic**: **Gradual progression**, **intermittent symptoms**, **conservative trial**
> ⭐ **Clinical Pearl**: **Dupuytren's contracture** affects **ring and little fingers** in **70% of cases** with **positive table-top test** indicating **surgical intervention**, while **trigger finger** shows **A1 pulley thickening** with **catching sensation** in **flexion-extension cycle**
**Fracture pattern analysis** distinguishes **stable vs unstable injuries** where **Bennett fractures** require **ORIF** due to **thumb metacarpal base instability**, **boxer's fractures** accept **angulation <40 degrees** in **5th metacarpal**, and **scaphoid fractures** need **immediate immobilization** regardless of **initial X-ray appearance** when **clinical suspicion** exists.
> 💡 **Master This**: **Gamekeeper's thumb** (UCL injury) demonstrates **>30 degrees angulation** or **>3mm opening** on **stress testing** indicating **complete rupture** requiring **surgical repair** - **Stener lesions** occur in **60% of complete tears** preventing **healing without surgery**
**Treatment response patterns** provide **diagnostic confirmation** where **infectious conditions** improve **within 48-72 hours** of **appropriate antibiotics**, **inflammatory arthritis** responds to **DMARDs over weeks-months**, and **mechanical problems** require **surgical intervention** when **conservative management fails after 3-6 months**.
Connect these **systematic discrimination principles** through **evidence-based treatment algorithms** to understand **optimal intervention timing** and **outcome prediction models**.
🔬 Systematic Analysis: Differential Diagnosis Architecture


⚡ Treatment Algorithms: Evidence-Based Decision Pathways
Treatment algorithms prioritize interventions based on functional impact where nerve injuries require immediate exploration when complete motor loss is present, tendon repairs achieve optimal results when performed within 7-10 days, and fracture stabilization prevents secondary complications when completed within 24-48 hours of injury.
📌 Remember: TIME HEALS WOUNDS - Tendon repairs best <7 days, Infections need immediate drainage, Microvascular repairs <6 hours, Extensor repairs <10 days - Hematomas evacuate <48 hours, Emergent nerve repairs <72 hours, Arterial repairs <6 hours, Lacerations close <12 hours, Stable fractures <7 days
Loading diagram…
Surgical technique selection follows evidence-based protocols where flexor tendon repairs use 4-strand techniques achieving gap resistance >40N with rupture rates <5%, nerve repairs employ microsurgical techniques with 10-0 sutures providing functional recovery in 70-80%, and fracture fixation utilizes plates and screws for unstable patterns achieving union rates >95%.
| Treatment Category | Technique | Success Rate | Complication Rate | Recovery Timeline |
|---|---|---|---|---|
| Flexor Tendon Repair | 4-strand core suture | 85-90% | Rupture 3-5% | Functional 3-6 months |
| Nerve Repair | Microsurgical technique | 70-80% | Neuroma 10-15% | Recovery 6-18 months |
| Fracture Fixation | Plate and screw | 95-98% | Infection 2-5% | Union 6-12 weeks |
| Replantation | Microsurgical anastomosis | 85-95% | Thrombosis 5-10% | Function 12-24 months |
| Tendon Transfer | Single transfer | 80-85% | Adhesions 15-20% | Strength 6-12 months |
⭐ Clinical Pearl: Replantation success depends on ischemia time where digits survive 12-24 hours cold ischemia but major limb segments require revascularization within 6 hours - venous congestion is more common than arterial thrombosis and requires immediate surgical revision
- Evidence-Based Treatment Hierarchies
- Acute Trauma Management
- Life-threatening: Hemorrhage control, airway management
- Limb-threatening: Vascular repair <6 hours, compartment release
- Function-threatening: Nerve repair <72 hours, tendon repair <7 days
- Chronic Condition Management
- Conservative trial: 6-12 weeks for most conditions
- Surgical intervention: Failed conservative or progressive symptoms
- Reconstructive options: Tendon transfers, joint fusion, arthroplasty
- Complication Management
- Infection: Immediate drainage, culture-directed antibiotics
- Non-union: Bone grafting, electrical stimulation
- Stiffness: Therapy trial, surgical release if >6 months
- Acute Trauma Management
Rehabilitation protocols integrate early mobilization where flexor tendon repairs begin passive motion day 3-5 using Kleinert protocols, nerve repairs start gentle ROM immediately to prevent stiffness, and fracture management allows early motion when stable fixation is achieved.
💡 Master This: Early mobilization protocols for flexor tendon repairs reduce adhesion formation by 40-50% compared to immobilization, but require patient compliance and therapist expertise - rupture rates increase to 8-12% with aggressive early motion versus 3-5% with controlled protocols
Outcome prediction models guide treatment selection where patient age >65 years reduces functional recovery by 20-30%, smoking increases complication rates by 2-3 fold, diabetes impairs wound healing and nerve regeneration, and worker's compensation cases show 30-40% lower satisfaction scores regardless of objective outcomes.
Understanding these treatment algorithms through multi-system integration reveals how surgical timing, technique selection, and rehabilitation protocols interact to optimize functional outcomes.
⚡ Treatment Algorithms: Evidence-Based Decision Pathways


🌐 Multi-System Integration: The Surgical Ecosystem
Systemic integration recognizes how metabolic conditions affect surgical outcomes where diabetes mellitus impairs wound healing by reducing collagen synthesis 30-40%, smoking decreases tissue oxygenation causing complication rates 2-3 times higher, and rheumatoid arthritis requires immunosuppression modification affecting infection risk and healing timelines.
📌 Remember: DIABETES DELAYS HEALING - Decreased collagen synthesis, Impaired angiogenesis, Altered immune function, Bacterial overgrowth, Elevated glucose, Tissue hypoxia, Endothelial dysfunction, Slow epithelialization
Microsurgical integration combines vascular surgery principles with plastic surgery techniques where vessel diameter matching within 0.5mm ensures optimal flow dynamics, nerve coaptation requires fascicular alignment and tension-free repair, and tissue transfer demands understanding of angiosomes and perfusion territories for flap survival rates >95%.
Loading diagram…
Anesthesia integration optimizes surgical conditions where regional blocks provide 8-12 hours pain relief with sympathetic blockade improving microcirculation, general anesthesia enables complex microsurgery requiring 4-8 hour procedures, and sedation protocols allow awake surgery for tendon transfers requiring active patient participation.
| Integration Aspect | Specialty Involved | Critical Parameters | Success Metrics | Failure Consequences |
|---|---|---|---|---|
| Metabolic Control | Endocrinology | Glucose <180mg/dL | Healing rate 90% | Infection risk 3x |
| Immunosuppression | Rheumatology | Steroid <10mg/day | Complication rate <15% | Healing delay 50% |
| Vascular Assessment | Vascular surgery | Perfusion pressure >50mmHg | Flap survival 95% | Tissue necrosis |
| Pain Management | Anesthesiology | VAS <4/10 | Mobilization day 1 | Stiffness 40% |
| Rehabilitation | Physical therapy | ROM >80% normal | Function score >80 | Disability 60% |
⭐ Clinical Pearl: Computer-assisted surgery using 3D planning and navigation systems improves screw placement accuracy by 85% in complex fractures and reduces operative time by 20-30% while decreasing radiation exposure for surgeon and patient
- Advanced Integration Technologies
- Imaging Integration: CT angiography, MR neurography, ultrasound guidance
- Real-time visualization: Vessel patency, nerve continuity, tendon gliding
- Surgical planning: 3D reconstruction, virtual surgery, implant sizing
- Monitoring Integration: Tissue oximetry, microdialysis, temperature monitoring
- Flap viability: Continuous assessment, early intervention, salvage protocols
- Infection detection: Biomarker monitoring, rapid diagnostics, targeted therapy
- Rehabilitation Integration: Motion analysis, force measurement, functional assessment
- Objective outcomes: ROM quantification, strength testing, activity monitoring
- Protocol adjustment: Real-time feedback, personalized therapy, goal modification
- Imaging Integration: CT angiography, MR neurography, ultrasound guidance
Research integration drives evidence-based advancement where multicenter trials establish treatment standards, biomechanical studies optimize surgical techniques, and outcomes research identifies predictive factors for functional recovery. Registry data from >10,000 procedures guides quality improvement and complication prevention.
💡 Master This: Integrated care pathways reduce hospital length of stay by 30-40%, decrease complication rates by 20-25%, and improve patient satisfaction scores by 15-20% through coordinated protocols, standardized communication, and multidisciplinary rounds
Future integration embraces artificial intelligence for diagnostic assistance, robotic surgery for precision enhancement, and telemedicine for remote monitoring - these technological advances promise improved outcomes while maintaining cost-effectiveness in hand surgery practice.
Connect these integration principles through rapid mastery frameworks to develop comprehensive clinical expertise and optimal patient care delivery systems.
🌐 Multi-System Integration: The Surgical Ecosystem


🏆 Clinical Mastery Arsenal: Rapid Reference Command Center
Essential Clinical Thresholds form the foundation of expert decision-making where specific numerical values guide immediate interventions and determine surgical timing. Master surgeons internalize these critical parameters enabling rapid assessment and confident treatment selection in emergency situations.
📌 Remember: CRITICAL NUMBERS SAVE HANDS - 6 hours: replantation limit, 12 hours: digit cold ischemia, 24 hours: warm ischemia limit, 48 hours: compartment syndrome window, 7 days: optimal tendon repair, 30 degrees: acceptable angulation, 3mm: instability threshold
Rapid Assessment Protocol enables systematic evaluation in <5 minutes identifying life-threatening, limb-threatening, and function-threatening injuries through structured examination and immediate decision trees.
- Master's Essential Arsenal
- Time-Critical Thresholds
- Replantation: <6 hours warm, <12 hours cold ischemia
- Compartment syndrome: Pressure >30mmHg or within 8 hours
- Arterial repair: <6 hours for limb viability
- Nerve repair: <72 hours for optimal outcomes
- Anatomical Landmarks
- No man's land: A1 to A5 pulley zone
- Danger zones: Guyon's canal, carpal tunnel, spiral groove
- Safe zones: Thenar crease, distal palmar crease
- Functional Thresholds
- Grip strength: >80% normal for return to work
- Pinch strength: >70% normal for fine tasks
- ROM: >80% normal for functional independence
- Time-Critical Thresholds
| Emergency Condition | Recognition Signs | Critical Action | Time Window | Success Rate |
|---|---|---|---|---|
| Compartment Syndrome | Pain out of proportion | Immediate fasciotomy | <8 hours | >90% if early |
| Arterial Injury | Absent pulse, pallor | Vascular repair | <6 hours | >85% patency |
| Complete Amputation | Tissue loss | Replantation | <12 hours cold | >90% survival |
| Open Fracture | Bone exposure | Irrigation, fixation | <24 hours | <5% infection |
| High-pressure Injection | Small puncture wound | Emergency exploration | <6 hours | >70% function |
| %%{init: {'flowchart': {'htmlLabels': true}}}%% | ||||
| flowchart TD |
START["<b>✋ Hand Emergency</b><br><span style='display:block; text-align:left; color:#555'>• Initial trauma</span><span style='display:block; text-align:left; color:#555'>• Acute hand injury</span>"]
ABC["<b>📋 ABCs Stable?</b><br><span style='display:block; text-align:left; color:#555'>• Airway/Breathing</span><span style='display:block; text-align:left; color:#555'>• Circulation check</span>"]
RESUS["<b>⚠️ Resuscitation</b><br><span style='display:block; text-align:left; color:#555'>• Stabilize FIRST</span><span style='display:block; text-align:left; color:#555'>• IV fluids/Oxygen</span>"]
BLEED["<b>📋 Bleeding Control?</b><br><span style='display:block; text-align:left; color:#555'>• Hemostasis check</span><span style='display:block; text-align:left; color:#555'>• Active hemorrhage</span>"]
PRESS["<b>💊 Pressure Control</b><br><span style='display:block; text-align:left; color:#555'>• Use tourniquet</span><span style='display:block; text-align:left; color:#555'>• Direct pressure</span>"]
NEURO["<b>📋 Neurovascular?</b><br><span style='display:block; text-align:left; color:#555'>• Pulse and sensation</span><span style='display:block; text-align:left; color:#555'>• Capillary refill</span>"]
EMERG["<b>⚠️ Emergency Surgery</b><br><span style='display:block; text-align:left; color:#555'>• Vascular repair</span><span style='display:block; text-align:left; color:#555'>• Revascularization</span>"]
OR6["<b>💊 OR in 6 Hours</b><br><span style='display:block; text-align:left; color:#555'>• Urgent OR time</span><span style='display:block; text-align:left; color:#555'>• Critical window</span>"]
FUNC["<b>📋 Function Loss?</b><br><span style='display:block; text-align:left; color:#555'>• Motor/Tendon check</span><span style='display:block; text-align:left; color:#555'>• Motion assessment</span>"]
URGENT["<b>🩺 Urgent Repair</b><br><span style='display:block; text-align:left; color:#555'>• Tendon/Nerve fix</span><span style='display:block; text-align:left; color:#555'>• Complete loss care</span>"]
OR24["<b>💊 OR in 24 Hours</b><br><span style='display:block; text-align:left; color:#555'>• Schedule surgery</span><span style='display:block; text-align:left; color:#555'>• Subacute repair</span>"]
ASSESS["<b>👁️ Systemic Eval</b><br><span style='display:block; text-align:left; color:#555'>• Further testing</span><span style='display:block; text-align:left; color:#555'>• Partial loss workup</span>"]
CONS["<b>✅ Final Plan</b><br><span style='display:block; text-align:left; color:#555'>• Conservative care</span><span style='display:block; text-align:left; color:#555'>• Or surgical fix</span>"]
START --> ABC
ABC -->|No| RESUS
ABC -->|Yes| BLEED
BLEED -->|No| PRESS
BLEED -->|Yes| NEURO
NEURO -->|No| EMERG
EMERG --> OR6
NEURO -->|Yes| FUNC
FUNC -->|Complete| URGENT
URGENT --> OR24
FUNC -->|Partial| ASSESS
ASSESS --> CONS
style START fill:#F7F5FD,stroke:#F0EDFA,stroke-width:1.5px,rx:12,ry:12,color:#6B21A8
style ABC fill:#FEF8EC,stroke:#FBECCA,stroke-width:1.5px,rx:12,ry:12,color:#854D0E
style RESUS fill:#FDF4F3,stroke:#FCE6E4,stroke-width:1.5px,rx:12,ry:12,color:#B91C1C
style BLEED fill:#FEF8EC,stroke:#FBECCA,stroke-width:1.5px,rx:12,ry:12,color:#854D0E
style PRESS fill:#F1FCF5,stroke:#BEF4D8,stroke-width:1.5px,rx:12,ry:12,color:#166534
style NEURO fill:#FEF8EC,stroke:#FBECCA,stroke-width:1.5px,rx:12,ry:12,color:#854D0E
style EMERG fill:#FDF4F3,stroke:#FCE6E4,stroke-width:1.5px,rx:12,ry:12,color:#B91C1C
style OR6 fill:#F1FCF5,stroke:#BEF4D8,stroke-width:1.5px,rx:12,ry:12,color:#166534
style FUNC fill:#FEF8EC,stroke:#FBECCA,stroke-width:1.5px,rx:12,ry:12,color:#854D0E
style URGENT fill:#F7F5FD,stroke:#F0EDFA,stroke-width:1.5px,rx:12,ry:12,color:#6B21A8
style OR24 fill:#F1FCF5,stroke:#BEF4D8,stroke-width:1.5px,rx:12,ry:12,color:#166534
style ASSESS fill:#EEFAFF,stroke:#DAF3FF,stroke-width:1.5px,rx:12,ry:12,color:#0369A1
style CONS fill:#F6F5F5,stroke:#E7E6E6,stroke-width:1.5px,rx:12,ry:12,color:#525252
> ⭐ **Clinical Pearl**: **High-pressure injection injuries** appear **deceptively minor** with **small entry wounds** but cause **extensive tissue damage** requiring **emergency exploration** and **debridement** - **delayed treatment >6 hours** results in **amputation rates >50%** versus **<10%** with **immediate intervention**
**Complication Management Protocols** provide **systematic approaches** to **common problems** where **infection** requires **immediate drainage** and **culture-directed antibiotics**, **non-union** needs **bone grafting** and **electrical stimulation**, and **stiffness** responds to **therapy** or **surgical release** depending on **duration** and **etiology**.
> 💡 **Master This**: **Flexor tendon rupture** after **repair** occurs in **3-8%** of cases, typically **10-14 days post-operatively** - **immediate recognition** and **re-repair within 48 hours** achieves **good outcomes in 70-80%** versus **<50%** with **delayed reconstruction**
**Outcome Optimization Strategies** integrate **patient factors**, **injury characteristics**, and **surgical techniques** to **maximize functional recovery** where **early mobilization**, **patient compliance**, and **therapist expertise** contribute **equally** to **final outcomes**.
🏆 Clinical Mastery Arsenal: Rapid Reference Command Center

Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more












Have doubts about this lesson?
Ask Rezzy, your AI Study Partner, to explain anything you didn't understand
Everything you need for NEET-PG prep
Get full Oncourse access with lessons, practice questions, flashcards and AI study tools.
Scan to download app