

CVD Risk Stratification - Spotting Trouble Early
- Goal: Identify high-risk individuals for targeted CVD prevention.
- Key Modifiable: Hypertension (HTN), Dyslipidemia, Diabetes Mellitus (DM), Smoking, Obesity (Asian BMI >23 kg/m²), Sedentary lifestyle.
- Indian Context: ↑Lp(a), ↑hs-CRP, Central Obesity (Waist: Men >90cm, Women >80cm), Low HDL.
- Tools: WHO/ISH charts (Indian adaptation), Framingham (less ideal for Indians), ASCVD Pooled Cohort Equations.
- Risk Tiers (10-yr CVD event):
- Low: <10%
- Moderate: 10-20%
- High: >20%
⭐ For the Indian population, target LDL cholesterol < 70 mg/dL in very high-risk individuals (e.g., established CVD, DM + multiple risk factors), and maintain BP < 130/80 mmHg.
Lipid & BP Targets - Numbers Game
- Lipid Targets (mg/dL):
- Very High Risk (ASCVD): LDL-C < 55; Non-HDL-C < 85
- High Risk: LDL-C < 70; Non-HDL-C < 100
- Moderate Risk: LDL-C < 100; Non-HDL-C < 130
- Triglycerides: Ideal < 150. Target if > 200 (Non-HDL-C), or if > 500 (pancreatitis risk).
- Statin Intensity:
- High (↓LDL ≥50%): Atorvastatin 40-80mg, Rosuvastatin 20-40mg
- Moderate (↓LDL 30-49%): Atorvastatin 10-20mg, Rosuvastatin 5-10mg
- 📌 High & Mighty: Atorva 40-80, Rosuva 20-40.
- BP Targets (mmHg) - General Indian Context:
- Standard Target: < 140/90.
- High-Risk (DM, CKD, ASCVD): < 130/80 (if tolerated).
- Age >65 yrs (not frail): SBP 130-139.
⭐ First-line antihypertensives (India): A (ACEi/ARB), C (CCB), D (Diuretics). β-blockers for CAD/HF.

Loading diagram…
Lifestyle Rx - Daily Dose Prevention
- Diet:
- Focus: Fruits, vegetables, whole grains, lean protein.
- Limit: Sodium (<2.3g/d), saturated/trans fats, added sugars.
- Key Diets:
Diet Focus Benefit DASH ↑F/V, low-fat dairy; ↓Na, fat ↓BP Mediterranean ↑F/V, nuts, olive oil, fish; ↓red meat CVD health
- Exercise:
- Aerobic: 150+ min moderate OR 75+ min vigorous/week.
- Strength: ≥2 days/week.
- Smoking: Cessation crucial. 5 A’s (Ask, Advise, Assess, Assist, Arrange).
- 📌 CVD risk ↓ significantly in 1 yr.
- Weight (Indians):
- BMI: <23 kg/m².
- Waist: ♂ <90cm, ♀ <80cm.
- Alcohol: Limit intake.
⭐ High refined carb/trans-fat Indian diets ↑CVD risk; traditional plant-based diets are protective.
Pharmaco-Prevention & Diabetics - Targeted Shields
-
Aspirin Therapy:
- Primary Prevention: 75-100 mg/day for select high ASCVD risk (e.g., 10-yr risk >20% or DM + multiple risk factors) & low bleed risk individuals. Indian guidelines emphasize careful selection.
- Secondary Prevention (established CVD): 75-100 mg/day (lifelong); often with P2Y12 inhibitor (e.g., Clopidogrel 75mg) post-ACS/PCI.
-
Diabetics & CVD Shielding:
- HbA1c goal: Generally <7%; individualize (e.g., <6.5% if new/young, <8% if elderly/comorbid).
- SGLT2 inhibitors (e.g., Empagliflozin 10/25mg, Dapagliflozin 10mg) & GLP-1 RAs (e.g., Liraglutide, Semaglutide) ↓CV events & mortality.
- Statins: Essential for most T2DM >40 yrs or with CVD risk factors.
-
Antiplatelet/Anticoagulant Choices (Prevention Focus):
Scenario Drug(s) of Choice Key Doses (daily) Primary Prevention (High ASCVD Risk) Aspirin 75-100 mg Secondary Prevention (Stable CAD) Aspirin ± Clopidogrel Asp: 75-100 mg, Clop: 75 mg AF (CHADS-VASc ≥2 M, ≥3 F) DOACs (Apixaban, Rivaroxaban) or Warfarin INR 2.0-3.0 for Warfarin -
Flowchart: Aspirin Primary Prevention (Indian Context)
Loading diagram…
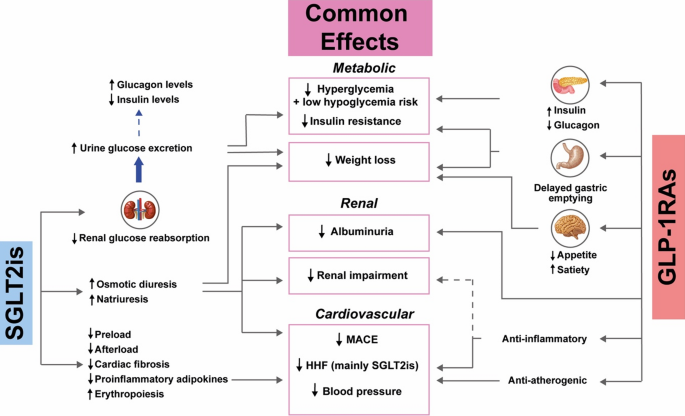
- ⭐ > Latest Indian guidelines recommend SGLT2 inhibitors or GLP-1 RAs for T2DM patients with established ASCVD or multiple risk factors, independent of HbA1c, for CV protection.
High‑Yield Points - ⚡ Biggest Takeaways
- Aspirin: Selective for primary prevention; essential for secondary prevention.
- Statins: Cornerstone for prevention; know high-intensity regimens (e.g., Atorva 40-80mg, Rosuva 20-40mg).
- Hypertension: Target <130/80 mmHg; lifestyle modifications are crucial.
- Diabetes Mellitus: Aggressive CV risk reduction; SGLT2 inhibitors & GLP-1RA provide CV benefits.
- Smoking cessation: Single most effective preventive strategy.
- Diet (DASH/Mediterranean) & Physical Activity (≥150 min/week moderate) are vital.
- Key Lipid Targets: LDL-C <70 mg/dL (secondary), <55 mg/dL (very high-risk).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more