

Lipoprotein Basics - Tiny Lipid Taxis
-
Function: Transport water-insoluble lipids (triglycerides, cholesterol, cholesteryl esters) in plasma.
-
Structure:
- Hydrophobic Core: Triglycerides (TG), Cholesteryl Esters (CE).
- Amphipathic Shell: Phospholipids, Free Cholesterol, Apolipoproteins.
-
Major Classes (listed by ↑density & ↓size):
- Chylomicrons (largest, least dense)
- VLDL (Very Low-Density Lipoprotein)
- IDL (Intermediate-Density Lipoprotein)
- LDL (Low-Density Lipoprotein)
- HDL (High-Density Lipoprotein; smallest, most dense)
-
Apolipoproteins (Apo): Proteins on the surface; roles in structure, receptor ligand binding, enzyme activation/inhibition (e.g., ApoA-I, ApoB-100, ApoC-II, ApoE).
⭐ ApoB-48 is unique to chylomicrons (intestinal origin), while ApoB-100 is found on VLDL, IDL, and LDL (hepatic origin).
Chylomicron Cycle - Gut to Liver Express
- Origin: Intestinal enterocytes package dietary TGs & cholesterol.
- Key Apolipoproteins:
- ApoB-48: Structural, unique to chylomicrons.
- ApoC-II: Acquired from HDL; activates Lipoprotein Lipase (LPL).
- ApoE: Acquired from HDL; ligand for liver remnant receptor.
- Transport Pathway:
- Gut: Nascent chylomicrons (ApoB-48) secreted into lymph.
- Blood: Mature by gaining ApoC-II, ApoE from HDL.
- Periphery: LPL (capillaries) hydrolyzes TGs → FFAs (to tissues) & glycerol (to liver).
- Remnant: Chylomicron Remnant (CR) forms, rich in cholesterol esters.
- Liver: CR binds ApoE receptor (LRP1) for endocytosis.
⭐ ApoB-48 is synthesized from the same gene as ApoB-100 via mRNA editing (C→U, creating a stop codon) in the intestine.

Loading diagram…
VLDL/LDL Journey - Liver's Delivery Service
Error: Failed to generate content for this concept group.
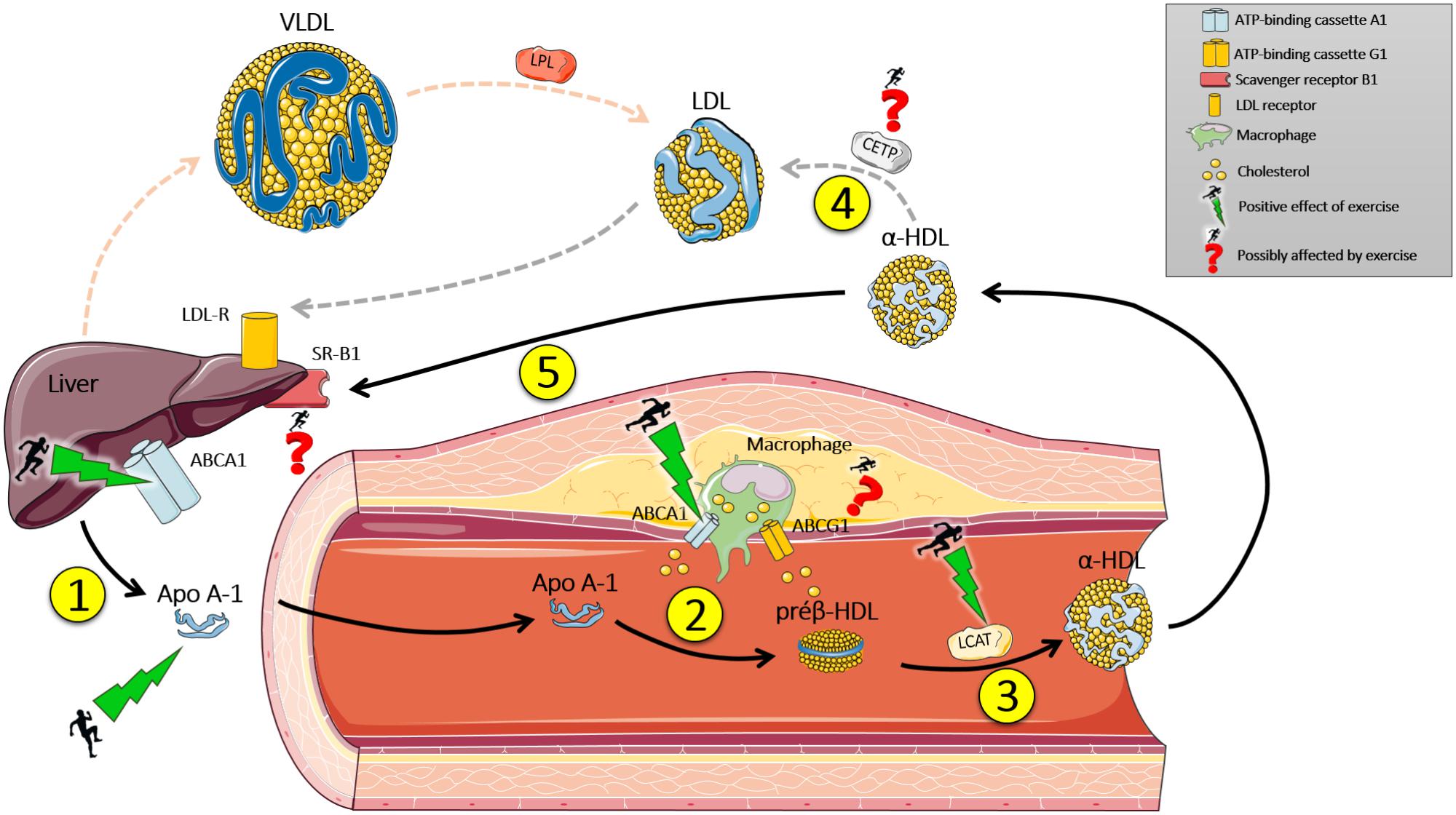
HDL's Good Deeds - Cholesterol Cleanup Crew
- HDL ("Good cholesterol"): Central to Reverse Cholesterol Transport (RCT); moves cholesterol from periphery to liver.
- Key Players:
- ApoA-I: Activates LCAT.
- LCAT: Esterifies free cholesterol (FC) $\rightarrow$ cholesteryl esters (CE) in HDL. $FC + Lecithin \rightarrow CE + Lysolecithin$.
- CETP: Exchanges HDL's CE for VLDL/LDL's TG.
- SR-B1: Hepatic receptor for HDL-CE uptake.
- ABCA1/ABCG1: Efflux FC from cells to HDL.
- RCT: Nascent HDL collects FC (ABCA1/G1) $\rightarrow$ LCAT esterifies $\rightarrow$ Mature HDL delivers CE to liver (SR-B1 or via CETP).
Loading diagram…
⭐ Low HDL-C (< 40 mg/dL ♂, < 50 mg/dL ♀) is a significant risk for coronary artery disease (CAD).
Lipid Disorders - When Taxis Crash
- Hyperlipidemias (HLP):
- Type I (LPL/ApoC-II def.): ↑Chylomicrons, ↑↑TG. Eruptive xanthomas.
- Type IIa (LDL-R def.): ↑LDL, ↑Cholesterol. Tendon xanthomas.
- Type IIb (FCHL): ↑LDL, ↑VLDL, ↑Cholesterol, ↑TG.
- Type III (ApoE def.): ↑IDL (remnants), ↑Cholesterol & TG. Palmar xanthomas.
- Type IV (FHTG): ↑VLDL, ↑TG.
- Hypolipidemias:
- Abetalipoproteinemia (MTP def.): ↓ApoB; malabsorption, acanthocytes.
⭐ Dysbetalipoproteinemia (Type III HLP) due to ApoE defect causes accumulation of chylomicron and VLDL remnants, presenting with pathognomonic palmar xanthomas.
High‑Yield Points - ⚡ Biggest Takeaways
- Chylomicrons: Transport dietary TGs; unique ApoB-48; largest size.
- VLDL: Carries endogenous TGs from liver; contains ApoB-100.
- LDL: Major cholesterol carrier to periphery ("bad"); ApoB-100 ligand for LDL receptor.
- HDL: "Good cholesterol"; reverse cholesterol transport; primary apolipoprotein is ApoA-I.
- Key Apolipoproteins: ApoA-I activates LCAT; ApoC-II activates LPL; ApoE for remnant uptake.
- Key Enzymes: LPL (TG hydrolysis); LCAT (cholesterol esterification in HDL); CETP (CE/TG exchange).
- Dyslipidemias: Familial Hypercholesterolemia (defective LDL receptors, ↑LDL-C).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more