

Lipoproteins & Metabolism - Fat Shuttles & Cycles
- Lipoproteins: Lipid carriers (Triglycerides - TG, Cholesterol).
- Chylomicrons (CM): Dietary TG transport. Key Apos: B-48, C-II, E.
- VLDL: Endogenous TG transport. Key Apos: B-100, C-II, E.
- IDL: VLDL remnant, LDL precursor. Key Apos: B-100, E.
- LDL: Cholesterol to tissues ("Bad"). Key Apo: B-100.
- HDL: Reverse cholesterol transport ("Good"). Key Apo: A-I.
- Key Players & Pathways:
- LPL (Lipoprotein Lipase): TG hydrolysis in CM/VLDL; activated by ApoC-II.
- LCAT (Lecithin-Cholesterol Acyltransferase): HDL maturation; activated by ApoA-I.
- CETP (Cholesteryl Ester Transfer Protein): Exchanges CE for TG between HDL & VLDL/LDL.
- ApoE: Ligand for hepatic uptake of CM remnants & IDL.

Loading diagram…
⭐ ApoE4 isoform: linked to ↑LDL-C, accelerated atherosclerosis, and ↑Cardiovascular Disease (CVD) risk. ApoE2 is associated with Type III hyperlipoproteinemia; ApoE3 is common/neutral.
Lipid Profile Components - Decoding the Numbers
- Total Cholesterol (TC): Overall cholesterol. Desirable: <200 mg/dL.
- LDL-C (Low-Density Lipoprotein Cholesterol): "Bad" cholesterol. Optimal: <100 mg/dL.
- Calculated by Friedewald formula: $LDL‑C = TC - HDL‑C - (TG/5)$ mg/dL (if TG <400 mg/dL).
- HDL-C (High-Density Lipoprotein Cholesterol): "Good" cholesterol. Protective: >60 mg/dL. Low (risk factor): <40 mg/dL.
- Triglycerides (TG): Normal: <150 mg/dL.
- VLDL-C (Very Low-Density Lipoprotein Cholesterol): Estimated as $TG/5$ mg/dL.
- Non-HDL Cholesterol: $TC - HDL‑C$. Secondary target. Desirable: <130 mg/dL.
⭐ Friedewald Formula Inaccuracy: Not valid if Triglycerides (TG) >400 mg/dL, chylomicrons present (non-fasting sample), or in Type III dyslipidemia (dysbetalipoproteinemia).
Dyslipidemias & Atherogenesis - When Lipids Rebel
- Dyslipidemia: Abnormal blood lipid concentrations (↑LDL-C, ↑Total Cholesterol, ↑Triglycerides, ↓HDL-C) that are key drivers for atherosclerosis.
- Classified as Primary (genetic, e.g., Familial Hypercholesterolemia) or Secondary (due to lifestyle, diabetes, hypothyroidism, nephrotic syndrome).
- Desirable Levels: LDL-C < 100 mg/dL (ideal < 70 or < 55 for very high-risk); HDL-C > 40 (Men) / > 50 (Women) mg/dL; Triglycerides < 150 mg/dL.
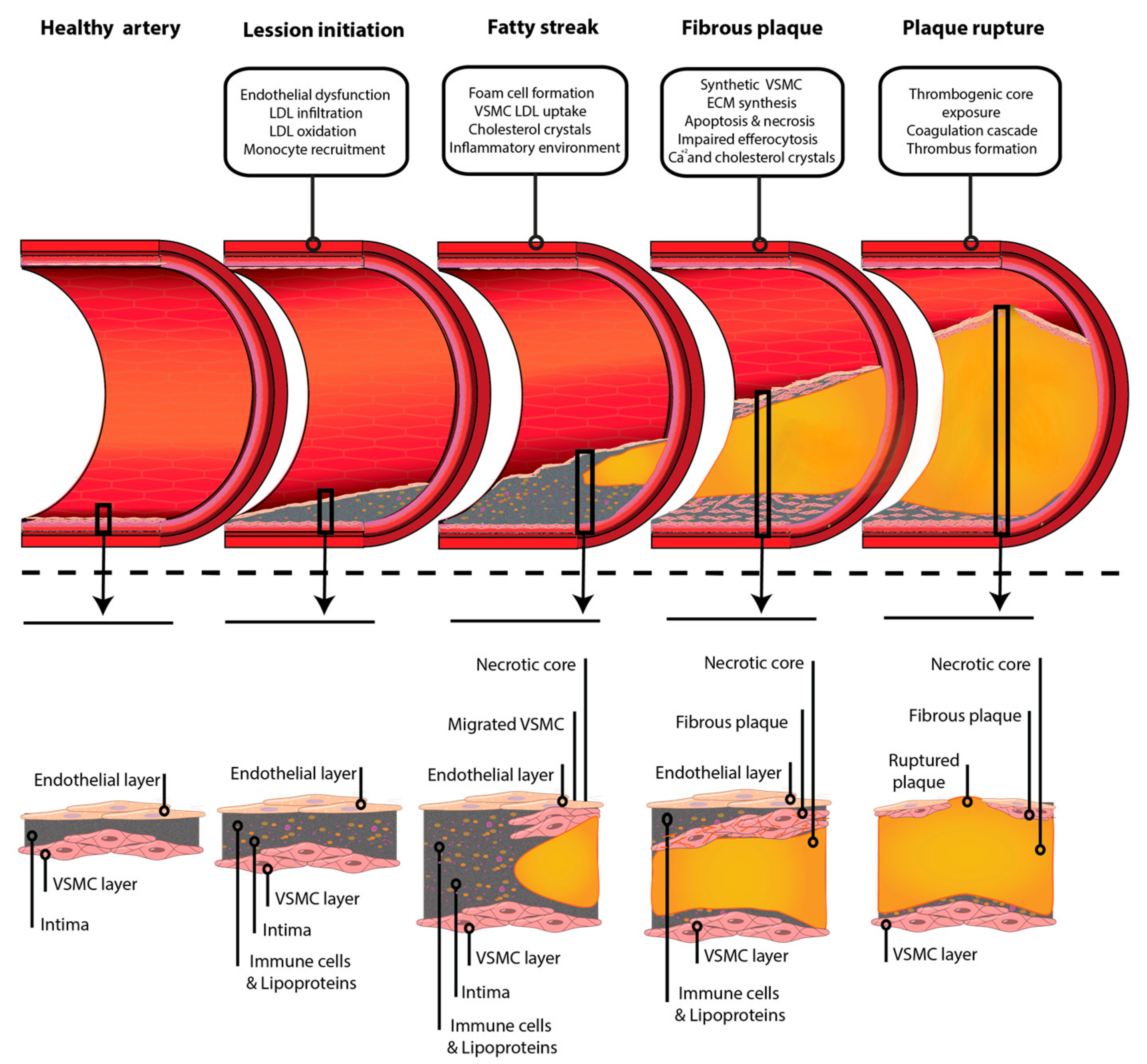
- Atherogenesis: The step-wise pathological process of plaque formation within arterial walls.
Loading diagram…
> ⭐ Lp(a), or Lipoprotein(a), is an independent, genetically determined risk factor for atherosclerotic cardiovascular disease (ASCVD), enhancing both atherogenesis and thrombotic risk.
CVD Risk & Management (India Focus) - Guarding the Heart
- Key Risk Factors (India Specific):
- Modifiable: Dyslipidemia (↑LDL-C, ↑Triglycerides, ↓HDL-C), Hypertension, Diabetes Mellitus, Smoking, Central Obesity (Waist: Men >90cm, Women >80cm), Physical inactivity, Unhealthy diet, ↑Lipoprotein(a) (>50mg/dL high risk).
- Non-Modifiable: Advancing Age, Family Hx of premature CVD, Male sex.
Loading diagram…
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more