

Joints & Bones - Joint Jamboree
- Bones: Framework for movement.
- Types: Long, Short, Flat, Irregular, Sesamoid.
- Parts: Epiphysis (articular cartilage), Diaphysis, Metaphysis.
- Joints (Articulations): Junctions between bones.
- Structural Classes: Fibrous (sutures), Cartilaginous (symphysis), Synovial (knee).
- Functional Classes: Synarthrosis (immovable), Amphiarthrosis (slight), Diarthrosis (free movement - all synovial).
- Synovial Joint Features:
- Articular cartilage (hyaline).
- Joint capsule (fibrous layer, synovial membrane).
- Synovial fluid (lubrication, nutrition).
- Ligaments (stability).

Loading diagram…
⭐ Hilton's Law: Nerves supplying muscles that cross and act on a joint also innervate the joint capsule and the skin over the joint.
Skeletal Muscles - Contraction Connection
- Sarcomere: Functional unit (Z-line to Z-line).
- A-band (Anisotropic): Myosin, some actin overlap; length constant.
- I-band (Isotropic): Actin only; shortens.
- H-zone (Heller): Myosin only; shortens.
- M-line: Center of H-zone.
- Sliding Filament Model: Thin actin filaments slide over thick myosin filaments. Myosin heads "walk" along actin.
- Excitation-Contraction (EC) Coupling: Links nerve impulse to muscle fiber contraction.
Loading diagram…
- Key Molecules & Structures:
- Ca²⁺: Binds troponin C, initiating contraction.
- ATP: Required for myosin detachment from actin and for SERCA pump activity.
- T-tubules: Propagate action potential into cell interior.
- Sarcoplasmic Reticulum (SR): Stores and releases Ca²⁺.
⭐ Malignant hyperthermia: rare, life-threatening reaction to anesthesia, often due to ryanodine receptor (RyR1) defects, causing sustained Ca²⁺ release and muscle rigidity.
Nervous Innervation - Nerve-Muscle Network
- Motor Unit: Fundamental functional unit; one α-motor neuron and all muscle fibers it innervates.
- Size principle: Smaller units recruited first for finer control (e.g., eye muscles); larger units for powerful movements (e.g., quadriceps).
- Neuromuscular Junction (NMJ): Specialized chemical synapse transmitting nerve impulse from motor neuron to muscle fiber.
- Key structures: Axon terminal (ACh vesicles), synaptic cleft, motor end plate (rich in nAChRs).
- Neurotransmission at NMJ:
Loading diagram…
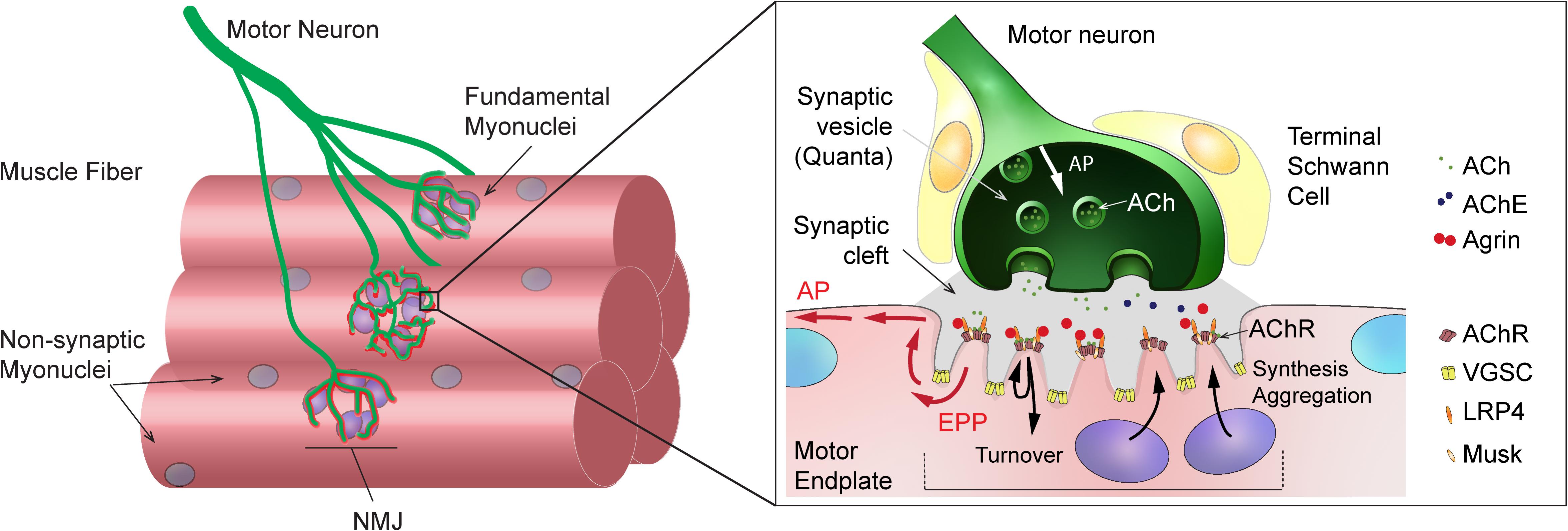
- Primary Neurotransmitter: Acetylcholine (ACh).
⭐ Myasthenia Gravis is an autoimmune disease where antibodies block or destroy nAChRs at the NMJ, leading to impaired neuromuscular transmission and muscle weakness.
Movement Principles - Lever Logic
- Lever System: Bone (bar), Joint (fulcrum F), Muscle contraction (effort E), Load (resistance R).
- Mechanical Advantage (MA): Ratio of effort arm to resistance arm. $MA = \text{EA} / \text{RA}$.
- Effort Arm (EA): Distance from fulcrum to effort application.
- Resistance Arm (RA): Distance from fulcrum to resistance application.
- Lever Classes (📌 Mnemonic: FRE 123 - Fulcrum, Resistance, Effort in middle for 1st, 2nd, 3rd class respectively):
- Class 1 (EFR/RFE): Fulcrum between E & R. E.g., Head nodding (atlanto-occipital joint). MA can be >, <, or = 1.
- Class 2 (ERF/FRE): Resistance between F & E. E.g., Plantarflexion (standing on tiptoes). MA > 1 (favors force).
- Class 3 (FER/REF): Effort between F & R. E.g., Elbow flexion (biceps). MA < 1 (favors speed/ROM).
⭐ Most levers in the human body are Class 3, designed for speed and range of motion rather than maximal force generation. This is crucial for activities requiring rapid movements like throwing or hitting.
High‑Yield Points - ⚡ Biggest Takeaways
- Lever Systems: Class 3 levers (e.g., biceps) most common, for speed/ROM. Class 1 for balance, Class 2 for force.
- Muscle Contractions: Isometric (static), Concentric (shortens), Eccentric (lengthens under load).
- Muscle Roles: Agonist (prime mover), Antagonist (opposes), Synergist (assists), Fixator (stabilizes).
- Motor Unit: A motor neuron and its muscle fibers; follows all-or-none law. Recruitment for graded force.
- Proprioceptors: Muscle spindles detect stretch. Golgi tendon organs detect tension.
- Movement Planes: Sagittal (flexion/extension), Frontal (abduction/adduction), Transverse (rotation).
Unlock the full lesson and continue reading
Signup to continue reading this lesson and unlimited access questions, flashcards, AI notes, and more