USMLE Step 3 Question Bank: Use Oncourse AI to Practice the Questions That Expose Weak Areas
Learn how to use USMLE Step 3 question banks as diagnostic tools to identify weak areas in clinical reasoning and management. Strategic review methods that go beyond passive practice.

USMLE Step 3 Question Bank: Use Oncourse AI to Practice the Questions That Expose Weak Areas
You have spent years learning to diagnose. Step 3 wants to know if you can manage.
The transition feels jarring at first. Instead of "What is the most likely diagnosis?", Step 3 asks "What is the next best step in management?" Instead of pattern recognition, it tests clinical algorithms. Instead of knowing facts, it demands knowing when to apply them.
Most residents approach their question bank like Step 2 CK — grinding through blocks, checking percentages, moving on. That wont work here. Step 3 question banks arent just practice engines. They are diagnostic tools that expose exactly where your clinical reasoning breaks down.
Here is how to use your Step 3 question bank as a weakness-finding system, not a passive score counter.
Why Step 3 Question Review Demands a Different Strategy
Step 3 isnt about what you know — its about what you do with what you know. Every question tests a clinical decision under pressure. Miss a question, and you have identified a gap in your management algorithms, not your knowledge base.
The exam structure reflects this reality. Day 1 tests foundational knowledge applied to primary care scenarios. Day 2 throws you into longitudinal patient management through Computer-based Case Simulations (CCS). Both days demand the same skill: translating clinical presentations into evidence-based actions.
Traditional question review fails because it treats wrong answers like knowledge gaps to fill. In Step 3, wrong answers usually reveal reasoning gaps to fix. You need to understand why you chose the wrong management step, not just memorize the right one.
The Step 3 Question Review Framework: Beyond Right and Wrong
When you miss a Step 3 question, classify the error first. Every wrong answer falls into one of five categories:
Content Gap: Missing a guideline, contraindication, or management sequence. This is the traditional "I dont know" error. Fix with targeted review. Algorithm Error: Knew the diagnosis but chose the wrong next step. You understand the condition but not the management sequence. Fix by mapping out decision trees. Context Misread: Correct knowledge applied to wrong setting. Outpatient pneumonia management in an ICU scenario, or emergency medicine approach in a primary care visit. Fix by practicing setting-specific reasoning. Risk-Benefit Miscalculation: Chose a plausible but inappropriate action due to risk-benefit assessment errors. Fix by reviewing when to be conservative vs aggressive. Process Error: Rushed reading, answer switching, or timing pressure. Fix with timed practice and reading discipline.Track these patterns. Content gaps require reading. Algorithm errors need flowchart practice. Context errors demand setting-specific drilling. Risk-benefit issues call for case-based reasoning. Process problems need mechanics work.
Most residents see only content gaps and try to read their way to improvement. Step 3 rewards algorithmic thinking over encyclopedic knowledge.
The Three-Column Error Log: Your Clinical Weakness Map
Create a simple spreadsheet with three columns for every missed question:
Column 1: Clinical Domain (Internal Medicine, Surgery, OB/GYN, Pediatrics, Psychiatry, Emergency Medicine, Preventive Care, Biostatistics, Ethics) Column 2: Task Type (Diagnosis, Management, Prognosis, Screening, Counseling, Quality Improvement, Patient Safety, CCS-style reasoning) Column 3: Specific Miss (What exactly went wrong)Example entries:
- IM | Management | CHF exacerbation — chose ACE inhibitor over diuresis in acute setting
- OB/GYN | CCS reasoning | Preeclampsia — missed magnesium sulfate for seizure prophylaxis
- Preventive | Screening | Mammography guidelines — mixed up age recommendations
Review your log weekly. Patterns emerge quickly. Maybe you consistently miss emergency management but nail outpatient decisions. Maybe you understand diagnoses but struggle with next-step sequencing. Maybe biostatistics questions always trip you up.
Each pattern points to a specific remedy. Emergency management needs algorithm practice. Next-step issues require decision-tree drilling. Biostatistics weakness calls for dedicated review of sensitivity, specificity, and study design concepts.
When using Oncourse AI for Step 3 practice, the Explanation Chat feature transforms your error log into active learning. After missing a management question, Explanation Chat turns your selected wrong answer into a targeted discussion thread. Instead of reading a static explanation, you can ask follow-up questions about why the correct management algorithm works and where your reasoning went wrong.
Converting Wrong Answers Into Repeatable Management Rules
Step 3 rewards pattern recognition at the management level. For each missed question, extract a concrete clinical rule you can apply to similar scenarios.
Dont write: "Preeclampsia requires monitoring."
Write: "Preeclampsia with severe features requires immediate magnesium sulfate, antihypertensive if BP >160/110, and delivery planning."
Dont write: "CHF patients need diuretics."
Write: "Acute CHF exacerbation: IV furosemide for volume overload, then optimize ACE inhibitor after stabilization."
Dont write: "Depression screening is important."
Write: "PHQ-2 for screening, PHQ-9 for monitoring, start SSRI if moderate-severe symptoms without contraindications."
Each rule should specify the trigger (clinical presentation), action (management step), and context (care setting). This builds the algorithmic thinking Step 3 demands.
For complex management sequences, Rezzy AI can help you create flowcharts and decision trees that stick. Ask it to map out antibiotic selection for pneumonia by setting, or hypertension management by stage and comorbidities. The visual format makes decision points clearer than text-based rules.
Weak Area Identification: From Symptoms to Systems
Step 3 organizes clinical content differently than Step 1 or Step 2 CK. Instead of learning by organ system, you need to think by clinical presentation and care setting.
Review your missed questions using this framework:
By Chief Complaint: Group errors by presenting symptom. Chest pain misses might span cardiology, pulmonology, and psychiatry. Abdominal pain errors could involve surgery, internal medicine, and OB/GYN. This reflects how Step 3 tests cross-specialty integration. By Care Setting: Emergency department questions demand rapid rule-out thinking. Outpatient questions reward conservative, cost-effective approaches. ICU scenarios require multisystem management. Preventive care questions test guideline knowledge and risk stratification. By Decision Type: Diagnostic questions ask what to test next. Management questions ask what to do next. Prognostic questions ask what to expect. Ethical questions ask what is appropriate. Each requires different reasoning patterns.Track your performance across these dimensions. You might excel at outpatient internal medicine but struggle with emergency psychiatry. You might nail diagnostic reasoning but falter at management sequencing.
For targeted practice on your weakest areas, use Oncourse AI's Step 3 question bank to create custom blocks focused on specific presentations or settings. The platform organizes questions by NBME blueprints, making it easy to drill weak domains.
CCS Practice Integration: Where Question Banks Meet Real Cases
Computer-based Case Simulations account for 25% of your Step 3 score, but most residents treat CCS as a separate skill from question bank practice. Big mistake. CCS cases are extended management questions with interactive interfaces.
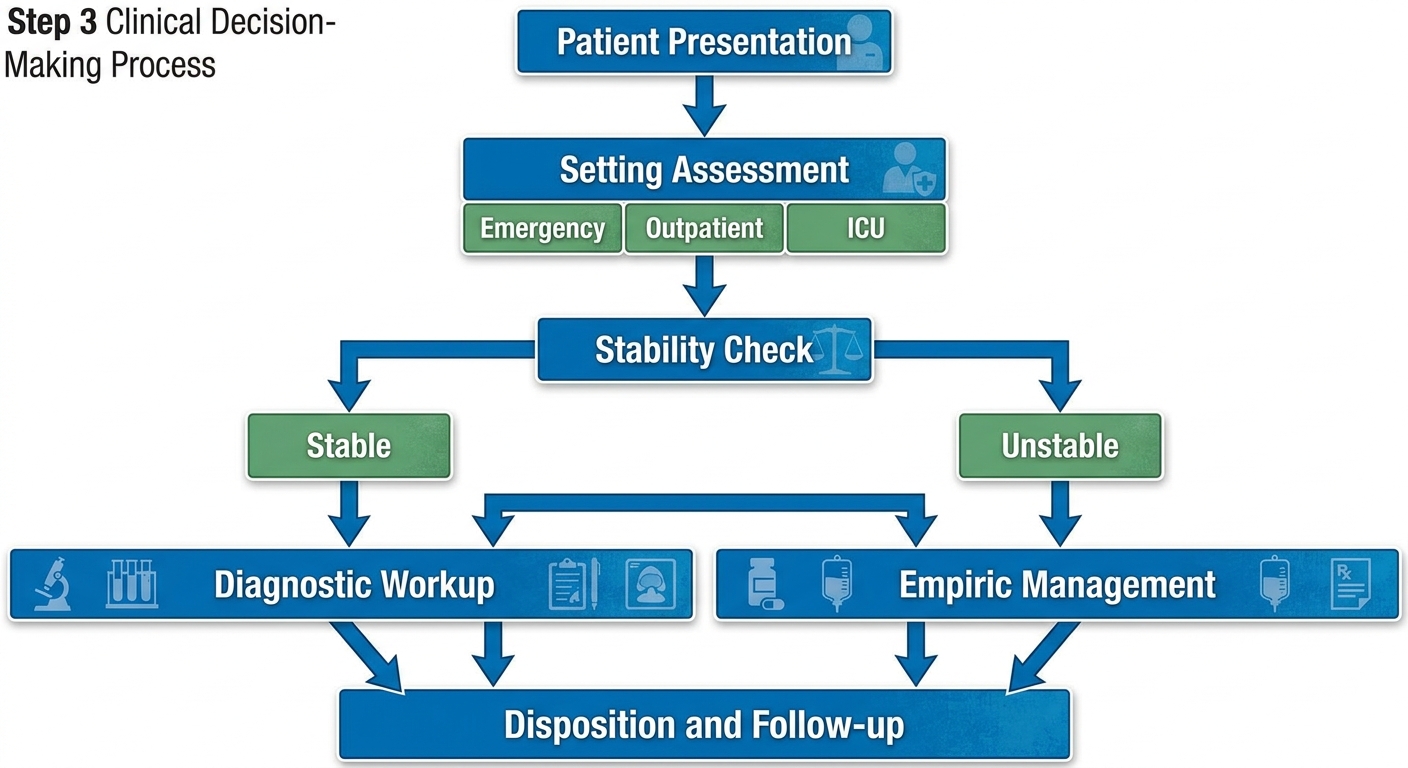
Every CCS case follows the same framework your question bank misses should reinforce:
1. Stabilize: ABCs, vital signs, immediate safety measures
2. Assess: Physical exam, initial workup based on presentation
3. Diagnose: Interpret results, narrow differential
4. Treat: Evidence-based management, monitor response
5. Disposition: Appropriate level of care, follow-up planning
Use your question bank errors to identify CCS practice targets. Miss pneumonia management questions? Practice pneumonia CCS cases. Struggle with CHF medication questions? Drill CHF CCS scenarios. The interfaces differ but the clinical reasoning patterns overlap.
When you miss a management sequence in a question block, translate that miss into CCS practice. If you chose the wrong antibiotic for pneumonia, practice CCS cases where you must select empiric coverage and adjust based on culture results. If you missed the timing of intervention in acute MI, practice CCS cases that test door-to-needle decision making.
Daily Practice Structure: Question Review as Active Diagnosis
Structure your question practice like clinical rounds. Each block should focus on a specific learning objective, not random sampling.
Monday Focus: Internal Medicine management across settings- 20-30 questions on IM topics from your weakness log
- Review errors immediately, extract management rules
- Practice related CCS cases if available
- High-acuity scenarios requiring rapid decision-making
- Emphasis on initial stabilization and disposition decisions
- Time pressure practice for Day 2 pacing
- Subspecialty management with primary care integration
- Age-specific and pregnancy-specific modifications
- Preventive care and counseling scenarios
- Communication skills and capacity assessments
- Quality improvement and patient safety scenarios
- Legal and ethical decision-making
- Study design interpretation and statistical analysis
- Screening guidelines and population health
- Evidence-based medicine application
- 40-60 question blocks simulating exam conditions
- Focus on domains from your error log
- Timed practice with immediate review
For residents using Oncourse AI, the platform's analytics automatically track your performance across these domains and suggest focus areas for each study session. Instead of guessing which topics need attention, you get data-driven recommendations that align with your actual weak spots.
Transforming Question Data Into Study Plans
Your question bank generates massive amounts of performance data. Most residents ignore this goldmine and focus only on overall percentages. Step 3 success comes from mining granular patterns.
Track these metrics weekly:
Domain Performance: Which medical specialties consistently challenge you? Setting Performance: Emergency vs outpatient vs inpatient success rates Question Length: Short vs long vignette accuracy patterns Time Pressure: Performance changes under timed vs untimed conditions Error Types: Knowledge vs reasoning vs process mistakesUse this data to build targeted study weeks. If emergency medicine management questions consistently trip you up, dedicate a week to EM algorithms. If long vignettes consistently challenge you, practice sustained attention and stem-reading discipline. If biostatistics questions show consistent weakness, block dedicated time for study design review.
Most importantly, track improvement trends. Are your target areas actually improving, or are you just repeating the same errors? If cardiology management questions remain problematic after two weeks of focused practice, change your approach. Maybe you need different resources, different practice formats, or different review methods.
When using Oncourse AI for Step 3 preparation, Rezzy can analyze your question patterns and create personalized mini-lessons on your weakest management algorithms. Instead of generic content review, you get targeted explanations of exactly where your clinical reasoning needs reinforcement.
The Two-Week Rapid Improvement Protocol
When you have identified consistent weak areas from your question bank data, implement this focused improvement protocol:
Week 1: Pattern Recognition- Day 1-3: 15 questions daily on weakest domain, untimed review
- Day 4-5: Map management algorithms for missed topics
- Day 6-7: Mixed practice with emphasis on weak areas
- Day 1-3: 20-25 timed questions on previously weak areas
- Day 4-5: CCS practice incorporating weak management sequences
- Day 6-7: Full-length mixed blocks to test improvement
For complex management algorithms that keep causing mistakes, create visual decision trees using simple flowchart tools or ask Rezzy to generate them for you. Visual organization makes decision points clearer and reduces the cognitive load during high-pressure questions.
Advanced Review Techniques: Beyond Explanation Reading
Reading explanations passively wont build the active reasoning skills Step 3 demands. After missing a question, try these active review methods:
Teach-Back Method: Explain the correct management sequence out loud as if teaching a medical student. Include the clinical reasoning, not just the facts. Alternative Scenario Creation: Change one variable in the question (patient age, setting, comorbidities) and determine how management would differ. Decision Point Mapping: For each management question, identify the key decision points that determined the correct answer. What clinical information drove the choice? Comparative Analysis: For questions with plausible incorrect choices, understand why each wrong answer fails. What makes the correct management step superior? Timing Analysis: For management sequences, understand the timing. What happens first, second, third? When do you reassess? When do you escalate?These techniques build the analytical reasoning patterns Step 3 rewards. You move from passive recognition to active clinical decision-making.
Frequently Asked Questions
How many questions should I do daily for Step 3?
Target 30-50 questions daily with thorough review. Quality matters more than quantity. Spend equal time practicing and reviewing. If you can only do 20 questions but review each thoroughly, thats better than 60 questions with superficial review.
Should I focus on my weakest areas or maintain strengths?
Focus 70% of your time on weakest areas, 30% on maintaining strengths. Step 3 rewards eliminating major weaknesses more than perfecting existing strengths. Use your question bank data to identify the areas dragging down your overall performance.
How do I know if I am ready for Step 3?
When your question bank performance shows consistent scores above your target across all major domains, and your error log shows decreasing frequency of repeat mistakes in management reasoning. Most importantly, when you can explain your reasoning for management questions, not just recall the right answers.
What percentage should I target in practice questions?
Aim for 70-80% on mixed question blocks. Step 3 has a lower pass threshold than Step 1 or Step 2 CK because it tests applied reasoning under time pressure. Focus on consistent performance across domains rather than peak percentages.
How should I integrate CCS practice with question bank work?
Use your question bank misses to guide CCS practice topics. If you miss pneumonia management questions, practice pneumonia CCS cases. Aim for 2-3 CCS cases daily in the month before your exam, focusing on your weakest clinical areas.
Should I review questions I got right?
Review questions you got right but felt uncertain about, or where you eliminated incorrect choices poorly. These reveal unstable knowledge that could fail under pressure. For confidently correct questions, brief review is sufficient.
Step 3 question banks are weakness-detection systems disguised as practice engines. Use them strategically, and they will show you exactly what clinical reasoning patterns need work. Ignore their diagnostic power, and you will keep repeating the same management errors under new disguises.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 3. Download free on Android and iOS.