Back
How to Study OB/GYN for USMLE Step 2 CK 2026: High-Yield Topics, Clinical Cases and Exam Strategy
Master USMLE Step 2 CK obstetrics gynecology with this comprehensive guide covering high-yield topics, clinical vignette strategy, and exam-focused study plans for 2026.

How to Study OB/GYN for USMLE Step 2 CK 2026: High-Yield Topics, Clinical Cases and Exam Strategy
You are staring at your Step 2 CK prep timeline. 280 questions. 8 hours. OB/GYN makes up 16-17% of those questions — that's roughly 45-47 questions that could make or break your score. Unlike Step 1's molecular focus, Step 2 CK obstetrics gynecology tests your clinical decision-making under pressure.
Here's what separates high scorers from everyone else: they dont treat OB/GYN like a memorization game. They master the clinical reasoning patterns that repeat across every vignette. Preeclampsia management. Ectopic pregnancy red flags. Labor progression algorithms. Contraceptive counseling.
This guide breaks down exactly how to tackle USMLE Step 2 CK obstetrics gynecology prep in 2026. You'll learn which topics carry the highest yield, how to decode clinical vignettes faster, and where to focus your limited study time for maximum point gain.
Understanding OB/GYN's Weight on Step 2 CK
OB/GYN questions on Step 2 CK aren't standalone knowledge checks. They're integrated clinical scenarios that test your ability to manage real patients under time constraints. The exam tests two core areas:
Obstetrics (60% of OB/GYN questions):
Prenatal care and screening
Pregnancy complications
Labor and delivery management
Postpartum care
Gynecology (40% of OB/GYN questions):
Reproductive health and contraception
Gynecologic disorders
Cancer screening
Sexual health and STIs
Each vignette presents a clinical scenario where you must identify the most appropriate next step in management, best initial diagnostic test, or most likely diagnosis. The key is recognizing patterns quickly and applying evidence-based protocols.
High-Yield OB/GYN Topics for Step 2 CK
Obstetrics: Pregnancy Complications (Highest Yield)
Preeclampsia and Hypertensive Disorders
This shows up in 8-10% of all OB/GYN questions. Know the diagnostic criteria cold:
BP ≥140/90 on two occasions 4+ hours apart after 20 weeks
With proteinuria (≥300mg/24hr or protein/creatinine ratio ≥0.3)
Severe features: BP ≥160/110, thrombocytopenia, elevated liver enzymes, renal insufficiency, pulmonary edema, new-onset headache/visual symptoms
Management algorithm: Mild preeclampsia at term → delivery. Severe preeclampsia → magnesium sulfate + delivery regardless of gestational age.
Ectopic Pregnancy
Classic presentation: 6-8 week amenorrhea + pelvic pain + vaginal bleeding. But watch for atypical presentations — shoulder pain from hemoperitoneum, or stable vitals masking internal bleeding.
Diagnostic approach: Transvaginal ultrasound if β-hCG >1500-2000 mIU/mL shows no intrauterine pregnancy. Serial β-hCG levels that plateau or fall suggest ectopic.
Postpartum Hemorrhage (PPH)
Defined as >500mL blood loss after vaginal delivery or >1000mL after C-section. Four causes (4 T's):
Tone (uterine atony) — 70% of cases
Trauma (lacerations, uterine rupture)
Tissue (retained placenta)
Thrombin (coagulopathy)
First-line: uterine massage + oxytocin. Refractory bleeding: methylergonovine, carboprost, or surgical intervention.
When practicing OB/GYN clinical vignettes, you can drill these exact scenarios using adaptive question sets that adjust difficulty based on your performance, helping you identify weak spots in pregnancy complication management.
Obstetrics: Normal Pregnancy and Labor
Prenatal Screening and Care
Know the timeline:
First trimester: Dating ultrasound, nuchal translucency, cell-free DNA testing
15-22 weeks: Maternal serum screening, anatomy ultrasound
24-28 weeks: Glucose tolerance test, Rhogam for Rh-negative mothers
35-37 weeks: Group B strep screening
Labor Management
Stage 1: Onset of labor to complete cervical dilation (10cm)
Latent phase: <6cm dilation, contractions every 5-20 minutes
Active phase: 6-10cm dilation, contractions every 2-3 minutes
Stage 2: Complete dilation to delivery of baby
Stage 3: Delivery of baby to delivery of placenta
Bishop score predicts successful induction: cervical dilation, effacement, station, consistency, position (max score 13).
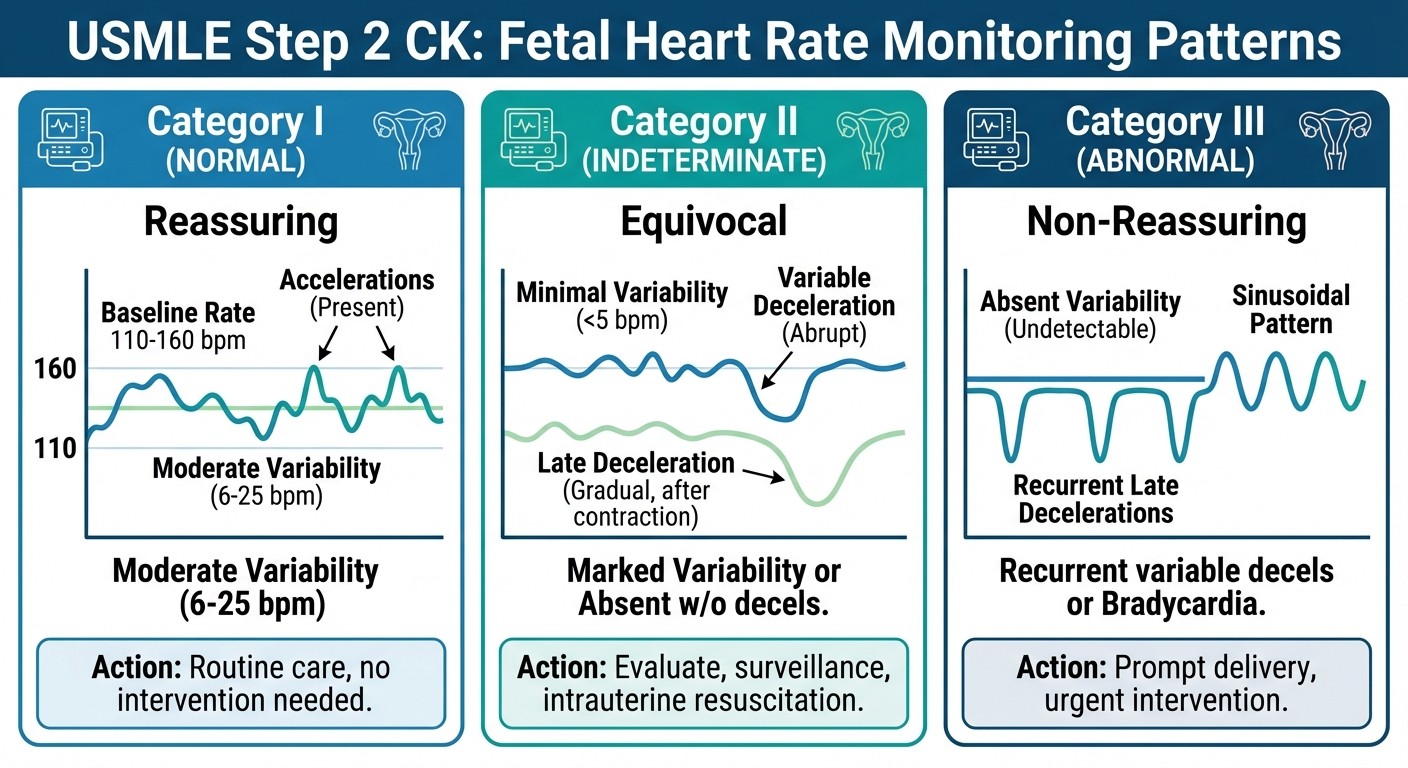
Fetal Monitoring
Category I (normal): Baseline 110-160 bpm, moderate variability, no concerning decelerations
Category II (indeterminate): Requires continued monitoring
Category III (abnormal): Sinusoidal pattern or recurrent late/variable decelerations with minimal variability → immediate delivery
Gynecology: Reproductive Health and Contraception
Contraceptive Methods
This appears in 6-8% of OB/GYN questions. Focus on contraindications and failure rates:
Combined OCPs contraindications: Age >35 + smoking, history of VTE, stroke, coronary artery disease, migraine with aura, active liver disease.
IUD considerations: Copper IUD effective for 10 years, can be used for emergency contraception up to 5 days post-unprotected intercourse. Levonorgestrel IUD reduces menstrual bleeding.
Menstrual Disorders
Primary amenorrhea: No menses by age 16 with normal secondary sexual characteristics, or by age 14 without secondary sexual characteristics.
Secondary amenorrhea: Absence of menses for 6 months in previously menstruating woman. Workup: pregnancy test → TSH, prolactin → progesterone challenge test.
Cervical Cancer Screening
2026 guidelines:
Ages 21-29: Pap smear every 3 years
Ages 30-65: Pap + HPV co-testing every 5 years OR Pap alone every 3 years
Post-hysterectomy: No screening if cervix removed for benign reasons
ASCUS with positive HPV: Colposcopy
ASCUS with negative HPV: Repeat co-testing in 3 years
The spaced repetition system helps lock in these screening timelines and management algorithms — you can flag complex cervical cancer scenarios from practice questions directly into review flashcard decks.
Gynecology: Common Disorders
Sexually Transmitted Infections
Chlamydia/gonorrhea: Often asymptomatic. Screen sexually active women <25 annually. Treatment: azithromycin + ceftriaxone for gonorrhea; azithromycin or doxycycline for chlamydia.
Bacterial vaginosis: Fishy odor, thin gray discharge, pH >4.5, positive whiff test, clue cells. Treatment: metronidazole.
Vulvovaginal candidiasis: Thick white discharge, vulvar itching, normal pH. Treatment: fluconazole or topical antifungals.
Pelvic Inflammatory Disease (PID)
Clinical criteria: Pelvic or abdominal pain + cervical motion tenderness OR uterine tenderness OR adnexal tenderness. No single test rules out PID.
Outpatient treatment: Ceftriaxone 250mg IM + doxycycline 100mg BID × 14 days + metronidazole.
Ovarian Masses
Premenopausal: Most are functional cysts. Complex masses or those >10cm need evaluation.
Postmenopausal: Any ovarian mass is concerning for malignancy.
CA-125 is elevated in ovarian cancer but also in endometriosis, fibroids, and PID — not specific for cancer screening in premenopausal women.
Clinical Vignette Strategy for OB/GYN
Reading the Stem Efficiently
Step 2 CK OB/GYN vignettes follow predictable patterns. Train yourself to identify the key elements within 30 seconds:
Patient Demographics: Age, gravidity/parity (G3P2 = 3 pregnancies, 2 deliveries), gestational age Chief Complaint: Bleeding, pain, fever, discharge, amenorrhea Physical Exam Findings: Vital signs, fetal heart rate, cervical exam, uterine size Lab Values: β-hCG, hemoglobin, urinalysis, cultures
Pattern Recognition for Common Scenarios
Heavy Menstrual Bleeding in Adolescent:
Think: anovulatory cycles due to immature HPO axis. First-line: OCPs or progestins.
Postmenopausal Bleeding:
Rule out endometrial cancer. Next step: transvaginal ultrasound → endometrial biopsy if endometrial thickness >4mm.
First Trimester Bleeding + Open Cervix:
Inevitable abortion. Management: expectant, medical (misoprostol), or surgical (D&C).
Second Trimester Loss + Painless Cervical Dilation:
Cervical insufficiency. Prevention in future pregnancies: cervical cerclage at 12-14 weeks.
Your performance on these pattern-recognition questions improves dramatically when you can track accuracy by subtopic — seeing that you're 62% accurate on gestational diabetes but 88% on contraception tells you exactly where to focus your next study session.
Time Management During the Exam
Each OB/GYN question should take 90 seconds maximum. Use this approach:
30 seconds: Read stem, identify key clinical scenario 45 seconds: Review answer choices, eliminate obviously wrong options 15 seconds: Select best answer based on standard management protocols
Dont get trapped in zebra diagnoses. Step 2 CK tests common presentations of common diseases.
Study Schedule and Resource Allocation
4-Week OB/GYN Intensive Plan
Week 1: High-Yield Obstetrics
Days 1-2: Pregnancy complications (preeclampsia, ectopic, gestational diabetes)
Days 3-4: Labor and delivery management
Days 5-7: Prenatal care and screening, practice questions
Week 2: High-Yield Gynecology
Days 1-2: Contraception and reproductive health
Days 3-4: Menstrual disorders and amenorrhea
Days 5-7: STIs and PID, practice questions
Week 3: Cancer Screening and Complex Cases
Days 1-2: Cervical, breast, and ovarian cancer screening
Days 3-4: Complex gynecologic disorders
Days 5-7: Mixed practice questions, review weak areas
Week 4: Integration and Simulation
Daily: 20-30 mixed OB/GYN questions
Review rationales for all incorrect answers
Focus on timing and pattern recognition
Daily Study Structure
Morning (45 minutes): Review new content using structured lessons Afternoon (60 minutes): Practice questions with immediate review Evening (30 minutes): Flashcard review of key algorithms and criteria
The key is active recall, not passive reading. Test yourself constantly. The adaptive question bank adjusts to your knowledge gaps, ensuring you spend time on concepts that actually need work rather than reviewing material you've already mastered.
Key Algorithms and Mnemonics
HELLP Syndrome Criteria
Hemolysis (LDH >600, schistocytes on smear) ELevated Liver enzymes (AST >70) Low Platelets (<100,000)
Apgar Scoring
Appearance (color): 0=blue/pale, 1=body pink/extremities blue, 2=completely pink Pulse: 0=absent, 1=<100, 2=>100 Grimace (reflex): 0=no response, 1=grimace, 2=cry Activity (tone): 0=limp, 1=some flexion, 2=active movement Respiration: 0=absent, 1=weak/irregular, 2=strong cry
Bishop Score Components
Dilation: 0=closed, 1=1-2cm, 2=3-4cm, 3=5+cm Effacement: 0=0-30%, 1=40-50%, 2=60-70%, 3=80+% Station: 0=-3, 1=-2, 2=-1/0, 3=+1/+2 Consistency: 0=firm, 1=medium, 2=soft Position: 0=posterior, 1=mid, 2=anterior
These mnemonics stick better when reinforced through spaced repetition flashcards — you can review Bishop scoring one day, Apgar the next, with the algorithm automatically surfacing cards you're about to forget.
Common Mistakes and How to Avoid Them
Diagnostic Pitfalls
Mistake: Ordering β-hCG in every reproductive-age woman Reality: Only order when pregnancy is clinically suspected based on history Mistake: Using CA-125 to screen for ovarian cancer Reality: CA-125 has poor specificity in premenopausal women Mistake: Treating every positive GBS culture Reality: Only treat GBS during active labor/ruptured membranes, not asymptomatic colonization
Management Errors
Mistake: Giving magnesium sulfate for mild preeclampsia Reality: Magnesium is only for severe preeclampsia or seizure prophylaxis Mistake: Treating partners for bacterial vaginosis Reality: BV is not sexually transmitted — only treat the patient Mistake: Immediate surgery for all ectopic pregnancies Reality: Methotrexate is appropriate for stable patients with β-hCG <5000 and mass <3.5cm
Question Strategy Mistakes
Mistake: Choosing the most complex management option Reality: Step 2 CK favors standard, evidence-based first-line treatments Mistake: Overthinking straightforward scenarios Reality: Common presentations get common management — trust the obvious answer
The most effective way to avoid these pitfalls is by practicing with immediate feedback on your reasoning, not just whether you got the answer right. Performance analytics show you which mistake patterns you repeat most often, so you can break bad habits before exam day.
Integrating OB/GYN with Other Step 2 CK Topics
OB/GYN doesn't exist in isolation on Step 2 CK. Expect integrated questions that test multiple specialties:
OB/GYN + Internal Medicine: Diabetic pregnant patient with poor glucose control OB/GYN + Pediatrics: Newborn complications from maternal conditions OB/GYN + Psychiatry: Postpartum depression screening and management OB/GYN + Emergency Medicine: Ectopic pregnancy with hemodynamic instability
Practice questions that cross specialty boundaries. These integrated vignettes often carry higher point values and separate top scorers from average performers.
Frequently Asked Questions
How much time should I spend on OB/GYN compared to other subjects?
Since OB/GYN represents 16-17% of Step 2 CK questions, allocate roughly 15-20% of your total study time. For an 8-week prep period, that's about 6-8 full study days dedicated to OB/GYN content.
Should I memorize normal lab values for pregnancy?
Yes, but focus on clinically relevant changes: physiologic anemia (Hgb 10-11 g/dL is normal), increased GFR leading to lower normal creatinine (<0.8 mg/dL), and gestational diabetes screening thresholds (1-hour glucose >140 mg/dL).
What's the best way to remember contraceptive contraindications?
Use categories: estrogen contraindications (VTE risk, stroke, MI, migraine with aura, liver disease), progestin contraindications (breast cancer, severe liver disease), and IUD contraindications (active PID, cervical cancer, severe immunocompromise).
How detailed should I know surgical procedures?
Focus on indications and contraindications, not surgical technique. Know when to recommend hysterectomy vs myomectomy for fibroids, but dont memorize suture types or approach details.
Is it worth studying rare genetic syndromes?
No. Step 2 CK emphasizes clinical decision-making for common conditions. Time spent on rare genetic syndromes is better invested in mastering preeclampsia management or contraceptive counseling.
How do I improve my timing on OB/GYN questions?
Practice with a timer and focus on pattern recognition. Most OB/GYN vignettes follow standard presentations — the sooner you recognize the pattern, the faster you can select the correct management approach.
Master OB/GYN for Step 2 CK Success
OB/GYN questions on Step 2 CK reward systematic preparation over last-minute cramming. Master the high-yield topics first: preeclampsia, ectopic pregnancy, normal labor progression, contraceptive management, and cervical cancer screening. These five areas alone account for 60-70% of OB/GYN questions.
Focus your practice sessions on clinical reasoning, not factual recall. Every vignette tests your ability to apply evidence-based protocols under time pressure. The students who score highest treat each practice question as a teaching case — analyzing not just what the correct answer is, but why the other options are wrong and what clinical pearls the question reveals.
Your Step 2 CK score depends on consistent, deliberate practice across all high-yield topics. Whether you have 2 weeks or 2 months to prepare, prioritize active learning methods that test your clinical reasoning in real time.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.