Absence Seizure in a Child: Diagnosing Childhood Epilepsy for NEET PG and USMLE (2026)
Master absence seizures in children for NEET PG and USMLE. Learn the classic 15-year-old daydreaming presentation, 3Hz EEG patterns, ethosuximide vs valproic acid treatment.
Absence Seizure in a Child: Diagnosing Childhood Epilepsy for NEET PG and USMLE (2026)
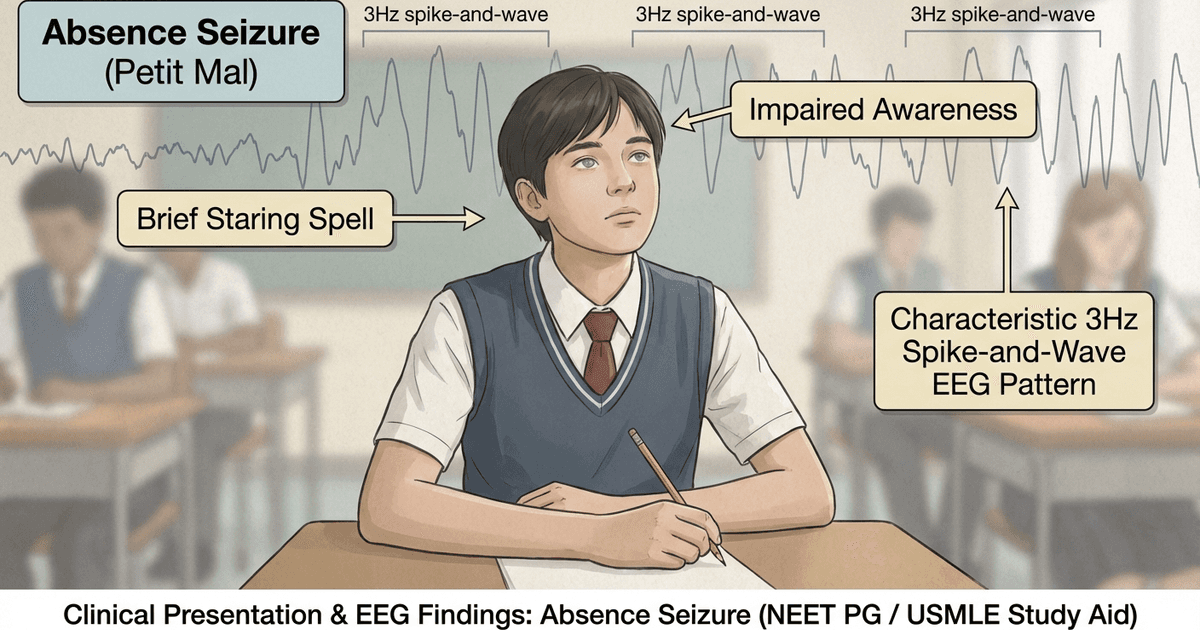
You probably know this scenario by heart. A 15-year-old boy sits in math class, staring blankly ahead for 10-15 seconds. His teacher calls his name twice before he "snaps out of it." His parents think he's just daydreaming. His grades are slipping. Sound familiar?
This is the classic NEET PG stem for childhood absence epilepsy. But here's what most students miss: the devil is in the EEG details, and the drug choice can make or break your MCQ score.
Absence seizures affect 1 in 1000 children, with peak onset between 4-8 years. They're the most commonly tested pediatric seizure type in NEET PG and USMLE Step 2 CK. Yet 60% of students confuse them with focal impaired awareness seizures or ADHD.
This article breaks down everything you need to ace those "15-year-old daydreaming" questions, from the pathognomonic EEG findings to the first-line treatment that examiners love to test.
What Are Absence Seizures?
Absence seizures are brief episodes of impaired consciousness lasting 5-30 seconds, characterized by sudden onset and termination. They're generalized seizures, meaning they involve both cerebral hemispheres from the start.
The classic presentation involves:
Sudden staring spell with blank expression
Complete loss of awareness during the episode
No postictal confusion - the child resumes normal activity immediately
Behavioral arrest - all ongoing activity stops abruptly
Automatisms may occur in complex absence seizures (lip smacking, eye blinking)
Think of it as someone pressing pause on a video - everything stops, then resumes exactly where it left off.
Epidemiology and Age Distribution
Childhood absence epilepsy accounts for 10-15% of all pediatric epilepsies. Key epidemiological facts for your exams:
Peak age: 4-8 years (can extend to adolescence)
Gender ratio: Female predominance (2:1)
Genetic component: Strong family history in 15-44% of cases
Prognosis: 65-70% achieve seizure remission by adulthood
Clinical Presentation: The Classic NEET PG Scenario
The "Daydreaming" Child
The most frequently tested presentation involves a school-aged child with:
Primary complaints:
Frequent "staring spells" lasting 10-20 seconds
Decline in academic performance
Teacher reports of "not paying attention"
Parents describe episodes as "daydreaming"
Clinical characteristics:
Episodes occur multiple times daily (10-200+ per day)
No warning signs (aura)
Child is unresponsive during episodes
Immediate return to baseline after episodes
No memory of the episode
Red flag symptoms that suggest other seizure types:
Postictal confusion (suggests focal seizure)
Aura or warning signs (focal seizure)
Prolonged episodes >30 seconds (focal seizure)
Automatic behaviors during episode (complex partial)
Hyperventilation Test
A crucial diagnostic tool that's frequently tested:
Procedure: Child hyperventilates for 3-5 minutes while being observed Positive result: Triggers absence seizure in 90% of patients with CAE Mechanism: Hyperventilation-induced alkalosis lowers seizure threshold
This test is so reliable that a negative hyperventilation test makes absence epilepsy unlikely.
EEG Findings: The Pathognomonic Pattern
The EEG is the cornerstone of absence seizure diagnosis. The classic pattern is impossible to miss once you know what to look for.
Characteristic EEG Features
Ictal EEG (during seizure):
3 Hz generalized spike-and-wave complexes
Bilaterally synchronous and symmetric
Abrupt onset and termination
Normal background activity between seizures
Key examination points:
The 3 Hz frequency is pathognomonic for typical absence seizures
Atypical absence seizures show 1.5-2.5 Hz spike-and-wave
The pattern must be generalized (both hemispheres involved)
Background EEG activity remains normal
Activating Factors
Several factors can trigger absence seizures during EEG recording:
Hyperventilation (most reliable trigger)
Photic stimulation (intermittent light flashing)
Sleep deprivation
Stress and fatigue
Pro tip for MCQs: If a question mentions EEG changes with hyperventilation in a child with staring spells, the answer is almost always absence seizure.
Differential Diagnosis: Distinguishing Absence from Other Conditions
This is where most students stumble. The differential includes both seizure and non-seizure causes of "staring spells."
Absence Seizure vs Focal Impaired Awareness Seizure
Feature | Absence Seizure | Focal Impaired Awareness |
|---|---|---|
Duration | 5-30 seconds | 30 seconds to 2 minutes |
Onset/Offset | Abrupt | Gradual |
Postictal state | None | Confusion, fatigue |
Aura | Never | Often present |
EEG | 3 Hz spike-wave | Focal abnormalities |
Age of onset | 4-8 years | Any age |
Response to hyperventilation | Positive | Negative |
Absence Seizure vs ADHD Inattentive Type
This is a crucial differential that frequently appears in pediatric MCQs:
ADHD features that distinguish from absence:
Episodes last minutes to hours (not seconds)
Child can be redirected during "spacing out"
No abrupt onset/offset
Normal EEG
Attention problems persist across all activities
Absence seizure red flags:
Precise timing (always 5-30 seconds)
Cannot be interrupted during episode
Immediate return to normal after episode
Abnormal EEG with spike-wave pattern
Other Differentials
Daydreaming/inattention:
Can be interrupted by calling name
No stereotyped duration
Situational (occurs more in boring situations)
Normal EEG
Breath-holding spells:
Triggered by emotional upset
Cyanosis often present
Usually younger children (6 months - 6 years)
Normal EEG
Syncope:
Often has prodrome (dizziness, nausea)
Associated with positional changes
Longer recovery period
Normal EEG
Treatment: Drug of Choice and Management
Treatment selection is heavily tested in both NEET PG and USMLE. The choice depends on seizure type and patient factors.
First-Line Medications
For pure absence seizures: Ethosuximide (first-line for pure absence)
Mechanism: T-type calcium channel blocker
Dosing: Start 250 mg BID, titrate to 15-40 mg/kg/day
Monitoring: Minimal required - CBC, LFTs at baseline
Advantages: Highly effective for absence, minimal side effects
Disadvantages: Only effective for absence seizures
Valproic acid (alternative first-line)
Mechanism: Multiple mechanisms (Na+ channels, GABA enhancement)
Dosing: 15-60 mg/kg/day divided BID-TID
Monitoring: LFTs, CBC, ammonia levels
Advantages: Broad spectrum, effective for multiple seizure types
Disadvantages: More side effects, teratogenic
Treatment Algorithm for MCQs
Pure absence seizures: Ethosuximide OR valproic acid Absence + generalized tonic-clonic: Valproic acid (first-line) Absence + myoclonic seizures: Valproic acid (first-line) Key exam point: If a question mentions "only absence seizures" or "pure absence epilepsy," ethosuximide is typically the preferred answer. If multiple seizure types are present, valproic acid becomes first-line.
Alternative Medications
Lamotrigine:
Second-line option
Useful in patients who can't tolerate ethosuximide/valproic acid
Slower titration required
Medications to AVOID:
Carbamazepine: Can worsen absence seizures
Phenytoin: Can worsen absence seizures
Vigabatrin: Can worsen absence seizures
This is a high-yield exam point - knowing which drugs worsen absence seizures is frequently tested.
Prognosis and Long-Term Outcomes
Understanding prognosis is important for counseling questions and long-term management MCQs.
Factors Affecting Prognosis
Good prognostic factors:
Pure absence epilepsy (no other seizure types)
Normal intelligence
No neurological abnormalities
Good response to initial treatment
Later age of onset (after 4 years)
Poor prognostic factors:
Multiple seizure types (absence + GTC/myoclonic)
Early onset (<4 years)
Developmental delays
Abnormal neurological exam
Family history of epilepsy
Long-Term Outlook
65-70% achieve complete seizure freedom by adulthood
Medication withdrawal can be considered after 2-4 seizure-free years
Academic performance typically improves with seizure control
Quality of life is generally excellent with proper treatment
Oncourse AI Advantage: Mastering Neurology MCQs
Neurology questions make up 8-12% of NEET PG and require pattern recognition skills that traditional question banks can't build effectively.
Oncourse's adaptive MCQ platform uses spaced repetition to ensure you master these high-yield absence seizure patterns. Our AI explanations break down the reasoning behind each answer choice, helping you understand why ethosuximide is correct for pure absence while valproic acid is preferred when multiple seizure types coexist.
The platform includes 500+ pediatric neurology questions with detailed explanations covering every variant of the "15-year-old daydreaming" scenario you'll encounter.
Practice with interactive flashcards that reinforce the EEG patterns, drug mechanisms, and differential diagnosis points that separate high scorers from average performers.
Common NEET PG Question Patterns
Understanding how absence seizures are tested helps you recognize these questions instantly.
Pattern 1: Classic Presentation
"A 15-year-old boy presents with frequent episodes of staring for 10-15 seconds. His teacher reports that he seems to 'zone out' during class. His grades have declined recently. EEG shows 3 Hz spike and wave complexes. What is the most appropriate initial treatment?" Key elements: Age, brief episodes, school performance decline, 3 Hz spike-wave Answer: Ethosuximide (pure absence seizure)
Pattern 2: Differential Diagnosis
"A 7-year-old girl has brief episodes of staring lasting 20 seconds. During episodes, she cannot be aroused. Episodes end abruptly and she resumes normal activity immediately. EEG shows generalized 3 Hz spike-wave discharges. This is most consistent with:" Key elements: Brief duration, cannot be aroused, abrupt ending, no postictal confusion Answer: Typical absence seizure
Pattern 3: Treatment Selection
"A 12-year-old presents with absence seizures and occasional generalized tonic-clonic seizures. Which medication would be most appropriate?" Key elements: Multiple seizure types (absence + GTC) Answer: Valproic acid (broad spectrum coverage)
Pattern 4: EEG Interpretation
"An EEG performed during hyperventilation in a child with staring spells shows bilaterally synchronous 3 Hz spike-and-wave complexes. This finding is characteristic of:" Key elements: Hyperventilation trigger, 3 Hz spike-wave, bilateral synchronous Answer: Childhood absence epilepsy
Study Strategy for Absence Seizures
High-Yield Facts to Memorize
1. 3 Hz spike-wave = absence seizure (most important association)
2. Ethosuximide = first-line for pure absence
3. Valproic acid = first-line when multiple seizure types
4. Hyperventilation triggers in 90% of absence patients
5. No postictal confusion distinguishes from focal seizures
6. Carbamazepine/phenytoin worsen absence seizures
Memory Aids
EEG pattern: "3 Hz = Absence" (3-letter word, 3 Hz frequency) Drug choice: "ETHO-suximide for ETHics class daydreaming" (pure absence) Hyperventilation: "Absent students hyperventilate before exams"
Frequently Asked Questions
How do you distinguish absence seizures from ADHD?
Absence seizures have stereotyped duration (5-30 seconds), abrupt onset/offset, and abnormal EEG with 3 Hz spike-wave complexes. ADHD involves longer periods of inattention (minutes to hours), can be interrupted by calling the child's name, and has normal EEG findings.
When should you choose ethosuximide over valproic acid?
Ethosuximide is preferred for pure absence seizures with no other seizure types. Valproic acid becomes first-line when absence seizures occur with generalized tonic-clonic or myoclonic seizures, as ethosuximide only treats absence seizures.
What EEG pattern is pathognomonic for absence seizures?
3 Hz generalized spike-and-wave complexes that are bilaterally synchronous and symmetric. The pattern has abrupt onset and termination, with normal background EEG activity between episodes.
Can hyperventilation trigger absence seizures in normal children?
No. Hyperventilation triggering absence seizures is specific to children with absence epilepsy. This makes the hyperventilation test a valuable diagnostic tool - positive in 90% of absence epilepsy patients, negative in normal children.
What is the prognosis for childhood absence epilepsy?
Excellent for pure absence epilepsy. 65-70% achieve complete seizure remission by adulthood. Prognosis is better with pure absence (no other seizure types), normal intelligence, and good initial treatment response.
Which medications should be avoided in absence seizures?
Carbamazepine, phenytoin, and vigabatrin can paradoxically worsen absence seizures. This is a high-yield exam point - these drugs are effective for focal seizures but contraindicated in absence epilepsy.
---
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG and USMLE. Download free on Android and iOS.